Research Article - (2015) Volume 4, Issue 2
Temporomandibular joint (TMJ) ankylosis is defined as bony or fibrous adhesion of the anatomic joint components accompanied with the mouth opening limitation. However, effective treatment method has not been still established. A 63-year-old man without dentofacial deformity visited our hospital with a complaint of limitation of mouth opening due to periarticular bone formation. His joints were possible of hinge movement; maximal incisal opening (MIO) was 17 mm. He refused surgical treatment. So he was treated mobilization therapy of TMJ when he visited our clinic and instructed to perform mouth-opening exercise by himself to prevent the progression of bony ankylosis. By successful of physical therapy, 6 months after, MIO was 28 mm. Limitation of mouth opening was not bothering him so much. After 9 years, periarticular tissue calcification was slightly progressive. But his joints of hinge movement were still remained. MIO was 25 mm. This case, physical therapy could be effective to prevent the progression from fibrous ankylosis of temporomandibular joint to the bony ankylosis.
Keywords: Temporomandibular joint; Ankylosis; Osteoarthritis; Physical therapy
TMJ is one of the most important joints in human body. It consisits of a condylar process of the mandible, glenoid fossa, articular disc and joint capsule. Two basic movments of the mandible be distinguished:the rotary or hinge movement and the translatory or sliding movment [1]. TMJ ankylosis is defined as bony or fibrous adhesion of the anatomic joint components accompanied with the mouth opening limitation. However, effective treatment method is not still established. Review or case reports of surgical treatments are publication [2-8]. But conservative treatment is rare reported. We reported a long followed up case of TMJ fibrous ankylosis treated with physical therapy.
In November 2004, a 63-year-old man visited our hospital with complaints of limitation of mouth opening and pain. He felt limitation of mouth opening without pain for 20 years.He had no dentofacial deformity and there was no past of the injury of the TMJ. His other joint movment was normal. Previous history is diabetic, dietetic treatment only. His family medical history of special note was none. MIO was 17 mm. Bilateral mandibular condyle could not move translocation or slide. His joints were possible of only hinge movement. Panoramic radiograph was revealed left TMJ bone malformation (Figure 1a). CT examination revealed morphological alteration in the articular fossa or condylar head at the bilateral side (Figures 2 and 3). Right TMJ was osteoarthritis (OA) change, an osteophyte was observed at the condylar head (Figure 2a). Left side, condylar head and glenoid fossa were showed severe cortical irregularities, in mandibular condyle and glenoid fossa. It was diagnosed fibrous ankylosis because of joint space visible (Figures 2b-2d and 3b, 3c).
He refused surgical treatment and hoped conservative therapy. So he was treated mobilization therapy of TMJ when he visited our clinic and instructed to perform self-mouth-opening exercise to prevent to changing of further bony ankylosis. Effect of conservative therapy, 6 months after, his mouth opening was showed significant improvement without pain. MIO was 28 mm. So limitation of mouth opening was not bothering him so much.
In May 2009, he felt limitation of mouth opening again, so visited our clinic again. MIO was 25 mm. Panoramic radiograph (Figure 1b) and CT examination revealed his left periarticular tissue calcification progressive, but joint space still visible as compared with in 2004 (Figures 2f, 2g and 2i)( Figures 3e and 3f). He refused surgical therapy and hoped to continue as treated conservative therapy. So we did mobilization therapy and instructed to performed self -mouth-opening exercise.
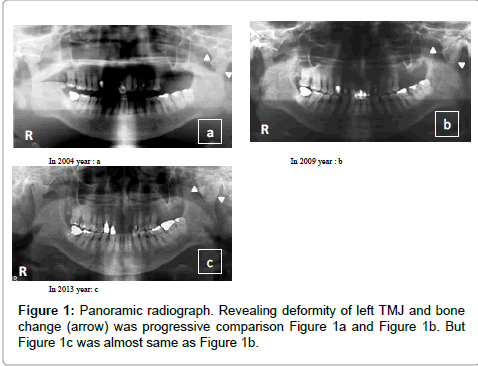
Figure 1: Panoramic radiograph. Revealing deformity of left TMJ and bone change (arrow) was progressive comparison Figure 1a and Figure 1b. But Figure 1c was almost same as Figure 1b.
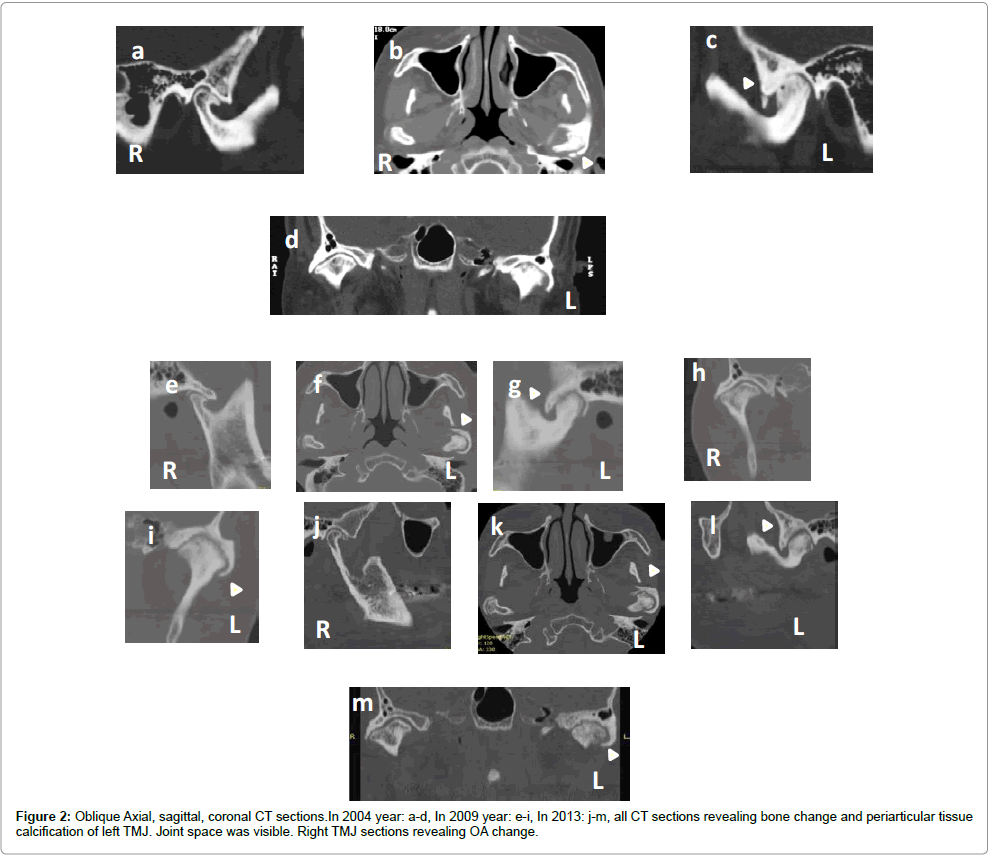
Figure 2: Oblique Axial, sagittal, coronal CT sections.In 2004 year: a-d, In 2009 year: e-i, In 2013: j-m, all CT sections revealing bone change and periarticular tissue calcification of left TMJ. Joint space was visible. Right TMJ sections revealing OA change.
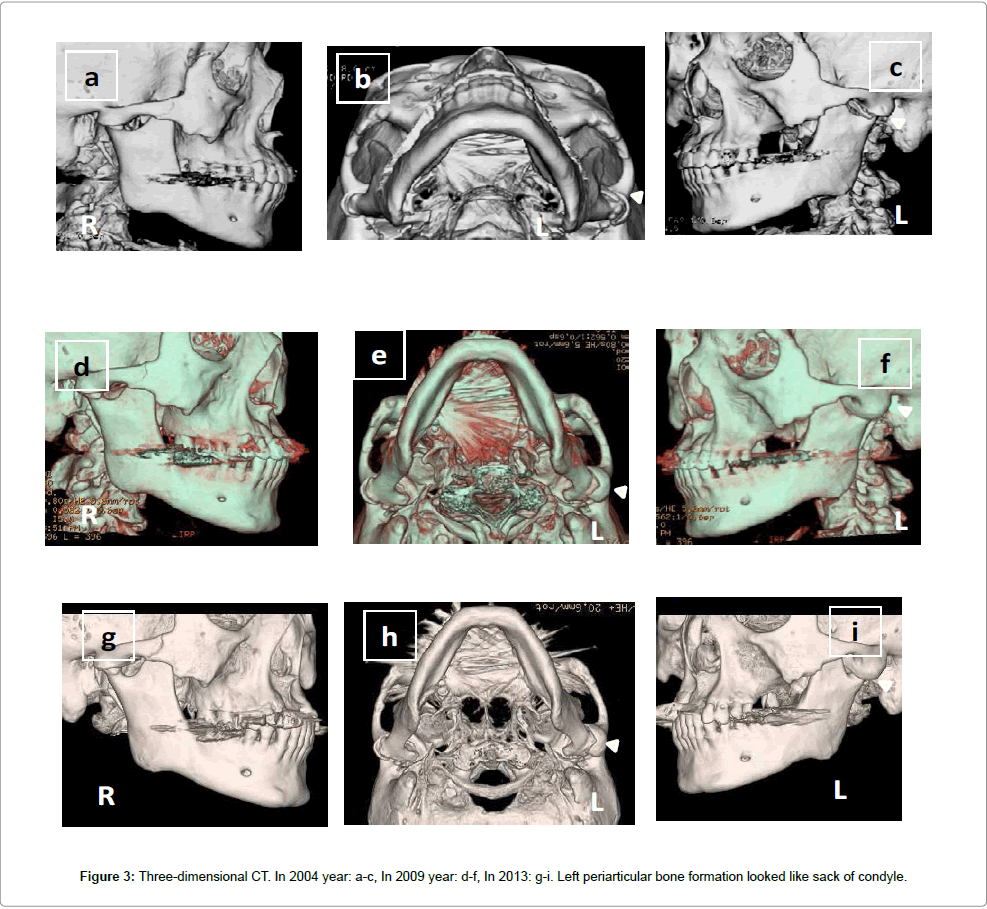
Figure 3: Three-dimensional CT. In 2004 year: a-c, In 2009 year: d-f, In 2013: g-i. Left periarticular bone formation looked like sack of condyle.
In March 2013, he felt left TMJ pain during the jaw-opening phase and could not eat and mouth opening without pain. MIO was 22 mm. So we treated him with mobilization therapy using selective COX-2 inhibitor (celecoxib: 200 mg twice daily) for 2 weeks and improvement of physical function. We did examination of panoramic radiograph (Figure 1c), MRI (Figure 4) and CT images (Figures 2 and 3). OA of right TMJ was stable (Figure 2a, 2e and 2j), left TMJ was joint space visible. It was still fibrous ankylosis (Figures 2k, 2l and 2m) and his bilateral condyles could be functioned of hinge movement. After 4 weeks, his pain was reduced, MIO was 25 mm.
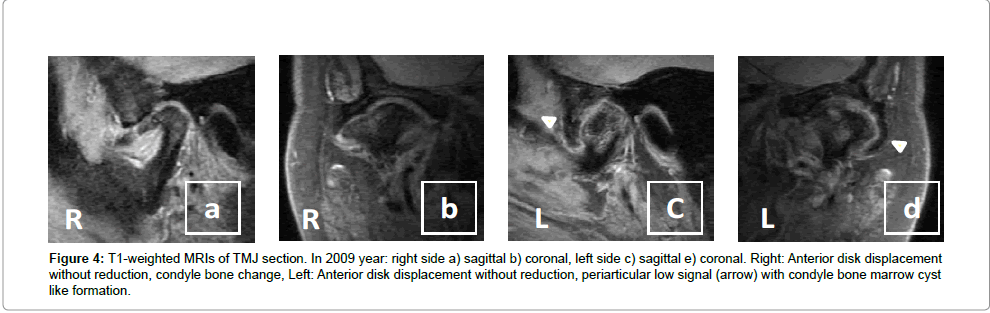
Figure 4: T1-weighted MRIs of TMJ section. In 2009 year: right side a) sagittal b) coronal, left side c) sagittal e) coronal. Right: Anterior disk displacement without reduction, condyle bone change, Left: Anterior disk displacement without reduction, periarticular low signal (arrow) with condyle bone marrow cyst like formation.
In October 2014, his joints were still functioned of hinge movement.
This case, there was no history of systemic disease and facial trauma, caused it to become ankylosis was unknown. In addition, patients were observed significant calcification in joint capsule corresponding parts in the literature search, was not observed in the jaw joints and other joints.
TMJ ankylosis is treated surgical treatment procedures include arthroplasy of joint cavity with or without a reconsturuction and a coronoidectomy, an autogenous costchondoral rib graft, distraction osteogenesis and intensive mouth-opening exercise, corrective orthognathic surgery or alloplastic joint protheses. Each method of surgical treatment is still failure rate high [2]. Sawhey [3] divided TMJ ankylosis 4 types in retrospect of the radio and operative findings. But it did not apply to our case. Durr [4] was reported post radiation therapy for preventive re-formation of heterotopic bone involving TMJ. Turlington-Durr classification to 4 grades of heterotopic ossification in the TMJ. Grade 2 was discription of periarticular bone formation. Only radiograh examination, but our case is semilar this heterotopic ossification. If TMJ ankylosis treats surgical procedure, it needs post self mouth-opening excesise for prevent re-ankylosis [5-8]. His first CT images, left joint space was visible. Temporomandibular disorders (TMD) patient’s physical therapy is effective [9]. This case could not improve mouth opening only physical therapy. But he refused surgical treatment, so we did physical therapy to prevent to change from fibrous adhesion to bony adhesions. While progress of left periarticular tissue calcification could not prevented, but bilateral joints space (between joint components) were remained. So his condyles could be functioned of hinge movment.
We experienced long follow up case of TMJ fibrous ankylosis. After 9 years, periarticular tissue calcification was slightly progress. But it was still functioned of hinge movement. This case indicates that it is important to start physical therapy at early stage of TMJ fibrous ankylosis and effective prevention of changing to bony ankylosis.
