Review Article - (2014) Volume 3, Issue 2
Ankle arthritis can be a painful and debilitating condition for many patients. In contrast to hip and knee arthritis, most cases of cases of symptomatic ankle arthritis are post-traumatic in nature. The anatomy, biomechanics and cell biology of the ankle differ from the hip and knee, and this has been postulated to account for the differing rates of post-traumatic vs. primary osteoarthritis in these joints. Non-operative treatment of ankle arthritis relies on antiinflammatory medication, intra-articular injections, and bracing. Patients with end-stage ankle arthritis who fail to respond to non-operative treatments benefit from ankle arthrodesis or total ankle replacement procedures
Keywords: Ankle arthritis, Osteoarthritis, Ankle joint, Ankle arthodesis
Osteoarthritis is associated with joint pain and dysfunction; and at late stages can result in joint contracture, muscle atrophy, and limb deformity [1,2] . It is the most common joint disease among middle aged and older individuals, and pain associated with arthritis is one of the more frequent reasons for seeking healthcare in this age group. Patients with end-stage ankle arthritis experience a high degree of functional impairment, and have been shown to have health related mental and physical disabilities as severe as patients with end-stage hip arthritis [3,4].
Limited data is available on the prevalence of ankle arthritis in the general population, but it is estimated to affect 1% of the population [5,6]. Patient visits for symptomatic hip and knee osteoarthritis are 9 to 10 times more common than those with ankle arthritis [2,5,7]. Primary osteoarthritis of the ankle is relatively uncommon, with post-traumatic arthritis accounting for more than 70% of cases of symptomatic ankle arthritis. This is approximately 7 times the rate of post-traumatic arthritis seen in the hip and knee [2,6,8]. In addition to ankle fractures, chronic ligamentous instability of the ankle has also been linked to long-term degeneration of the joint [6,9,10]. In a study of 390 patients with symptomatic ankle arthritis, Valderrabano found a 78% rate of post-traumatic ankle arthritis. In this series, malleolar fracture accounted for 39% of post-traumatic cases with ligamentous injuries and pilon fractures accounting for 16% and 14% respectively [6]. Less common causes of ankle arthritis include: infection, tumor, hemochromatosis, neuropathic arthropathy, inflammatory arthritis and crystalline arthropathy [11].
Several anatomic, biomechanical, and biochemical factors are thought to make the ankle joint more susceptible to post traumatic arthritis while being more resistant to primary osteoarthritis.
The ankle joint is formed by the distal articulation of the tibia and fibula with the talus. The boney and ligamentous restraints of the ankle mortise confer a high level of stability to the ankle joint. When compared to the knee, the ankle experiences less overall range of motion, and is subject to less gliding and rotational motion. In addition, the shape of the tibio-talar articulation allows for a high degree of surface congruency during weight bearing. These differences have been postulated to predispose the knee to a higher incidence of primary osteoarthritis [12].
The ankle acts as the first major articulation responsible for transferring ground reactive forces, and during normal level walking, experiences loads that are 5 times body weight [13]. Despite the high demands placed on the ankle joint, it has a smallest area of contact of the major lower extremity joints during normal loading (350 mm2 compared to 1,120 mm2 and 1,100 mm2 in the hip and knee, respectively) [14-16]. The ankle also has the thinnest and most uniform cartilage of all the major lower extremity joints, ranging from 1 to 1.7 mm, compared to knee cartilage, ranging from 1 to 6 mm in thickness [17,18]. Ankle cartilage has also been shown to be stiffer with a greater mean compressive modulus than the thicker hip and knee articular cartilage [19]. Additionally, differences in age related changes to articular cartilage have been demonstrated among the lower extremity joints. One study showed that tensile fracture stress and stiffness of ankle articular cartilage deteriorated less rapidly than hip articular cartilage with advancing age. The authors of this study postulated that this reduction in tensile properties in hip cartilage could partially explain the increased rate of primary osteoarthritis in the hip as compared to the ankle [20].
In a review of the literature on knee and ankle cartilage properties, Hendren et al. noted several recognized differences in their biochemical, cellular and metabolic properties. Ankle articular cartilage was noted to be more cellular, with cells grouped into chondrons, possibly allowing for better intercellular signaling. Ankle cartilage was also thought to be more resistant to inflammatory molecules such as Il-1. In addition, chondrocytes were found to have increased metabolic activity in the ankle [21].
Clear differences in anatomy, biomechanics and cartilage properties between the ankle and other lower extremity joints exist. The significance of these differences has not been fully elucidated with the respect to the differing rates of post traumatic and primary osteoarthritis. A better understanding of how these properties relate to the development of arthritis will be necessary for the development of more effective and preventative treatments.
In most patients, symptoms of ankle arthritis will present insidiously, and may initially wax and wane over time. Non-operative treatments may help provide pain relief and improve function in this early stage of the disease. The most common forms of non-operative treatments include bracing, analgesic and anti-inflammatory medications, and intra-articular injections. Despite our reliance on non-operative treatments in the early stages of ankle arthritis, high quality evidence is lacking to support most of these treatment modalities.
Braces and assistive devices have long been considered as a first line option for treatment of painful arthritic conditions. The reduction of ankle motion and joint reactive forces at the ankle is the primary goal of bracing and shoe modifications. These devices may produce a beneficial effect for those patients who have symptoms primarily with ambulation. Several bracing options have been recommended for patients with ankle arthritis. An ankle foot orthosis limits movement at the ankle joint and theoretically reduces pain associated with motion at the arthritic joint [22,23]. Other options include a rocker sole and solid ankle cushion heel (SACH) orthosis for treatment of ankle arthritis. This device has been shown to both decrease ankle motion and help transition from heel strike to toe off during walking [23,24]. In addition to bracing, assistive devices are a useful adjunct to decrease forces at the ankle joint. The use of a cane has been shown to effectively offload as much as 25% of one’s bodyweight, thus reducing joint reactive forces at the ankle [23,25]. While older patients may tolerate bracing and assistive devices, younger patients are usually more resistant to longterm use of these devices due to cosmetic concerns or social stigma.
Medicinal therapy comes in the form of oral non-steroidal antiinflammatory drugs (NSAIDs), acetaminophen (APAP), and topical NSAIDs. Oral acetaminophen and NSAIDs are widely available, and are commonly used by patients as a first line treatment for osteoarthritis. However, many experts still remain divided on the efficacy of the two drugs in the treatment of osteoarthritis. Many major clinical guidelines recommend APAP as the initial treatment for mild to moderate osteoarthritis related pain due to its low side effect profile [26]. However, in a systematic review of acetaminophen for osteoarthritis, Towheed et al concluded that NSAIDs were superior to APAP in improving osteoarthritis related hip and knee pain [27]. To our knowledge, there have not been any high quality studies evaluating these drugs efficacy, specifically for the treatment of ankle arthritis.
Topical NSAIDs have increased in popularity in recent years as the concerns over the gastrointestinal, renal, and cardiovascular side effects associated with oral NSAIDs have come to the forefront. Studies have shown that topical diclofenac application results in lower systemic concentrations than with oral administration [28]. In a systematic review of the literature, Derry et al. concluded that topical diclofenac was at least as effective as oral diclofenac for hand and knee osteoarthritis, and likely as effective as other oral NSAIDs. In their review they found local skin irritation to be the most common side effects associated with topical NSAIDs use [29]. Topical NSAIDs are available over the counter outside the U.S. and are accepted as a first line treatment for musculoskeletal pain. While little evidence is offered for the specific use of these agents for the treatment of pain related to ankle arthritis, we have found them to be a good first line option for treatment in patients who do not tolerate oral NSAIDs.
Intra-articular injections come in the form of corticosteroids and viscosupplementation. Intra-articular injections of steroids into the ankle are considered to reduce pain and inflammation. In the knee, corticosteroid injections for arthritis have produced short-term relief (8 weeks) of arthritis symptoms [30,31]. However, limited evidence is available on the effectiveness of corticosteroid injections for ankle arthritis [32,33]. We find this treatment to be a useful option for patients who have failed medicinal therapy. In addition, when steroid injection is combined with a local anesthetic, it also serves as a diagnostic adjunct to confirm the source of pain in patients with atypical symptoms.
Viscosupplementation in the form of hyaluronic acid is the second option for intra-articular injection. A small number of studies have addressed the use of hyaluronic acid for the treatment of ankle arthritis. Two randomized studies compared five weekly injections of a low-molecular weight, non-cross-linked-hyaluronic acid product (Hyalgan) with a saline control. These studies found no difference in AOS and VAS scores between the groups at 6 months follow up [34,35]. A more recent randomized double blinded placebo controlled study of a single injection of non-cross-linked haluroic acid (Supartz) also failed to produce a significant difference in AOFAS scores at 6 and 12 weeks [36]. While different preparations and dose regimens deserve further study, we currently do not find viscosupplementation to be useful for the treatment of ankle arthritis.
The most widely accepted surgical treatments for end stage ankle arthritis are arthrodesis and ankle replacement. Less common and more controversial options include: distraction arthroplasty, supramalleolar osteotomy, interposition arthroplasty, and bipolar allograft ankle arthroplasty. In this review we will focus on ankle arthrodesis and total ankle arthrosplasty.
Ankle arthrodesis was first described for treatment of paralytic foot and ankle deformities in the late 19th and early 20th centuries. It wasn’t until the 1930s that ankle arthrodesis procedures were recognized as an option for the treatment of painful ankle fracture malunions with joint incongruity [37]. Ankle arthrodesis has since gained acceptance as the gold standard for treatment of painful ankle arthritis that has failed non-operative management.
The goal of ankle arthrodesis is to produce a stable boney fusion at the tibio-talar articulation (Figure 1). The procedure involves debridement of articular cartilage, preparation of subchondral bone, and application of stable fixation across the fusion site. In 1951, Charnely introduced the concept of compression arthrodesis using an external fixation device, which was a major technical advance at the time [38]. Modern methods of stabilizations include external fixation, internal fixation with screws alone, and internal fixation with plate and screw constructs. In the absence of a compromised soft tissue envelope, most surgeons will prefer some form of rigid internal fixation to stabilize the arthrodesis. This strategy has been successful with most studies reporting union rates of 90% or higher when rigid internal constructs are used [34,36,38].
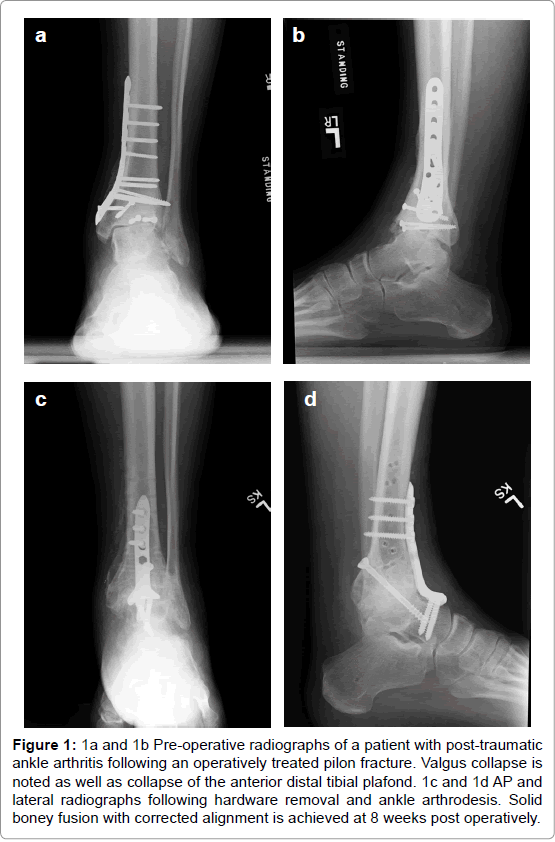
Figure 1: 1a and 1b Pre-operative radiographs of a patient with post-traumatic ankle arthritis following an operatively treated pilon fracture. Valgus collapse is noted as well as collapse of the anterior distal tibial plafond. 1c and 1d AP and lateral radiographs following hardware removal and ankle arthrodesis. Solid boney fusion with corrected alignment is achieved at 8 weeks post operatively.
The optimal position for fusion has been borne out in a number of gait studies. It is recommended that the ankle be fused in 5 degrees of valgus, 5 to 10 degrees of external rotation and neutral flexion. Optimal position of the ankle arthrodesis is essential for a good functional outcome [39-42].
Short-term results of ankle arthrodesis have been good, with improvement in pain, self-reported clinical outcome scores, and gait parameters [43-46]. In addition, the rate of complications after ankle arthrodesis is low with the primary reason for revision in most series being non-union [47,48]. Long term follow up studies (mean >20 yrs) have also shown good results, with most patients maintaining a high level of satisfaction with their ankle fusion, despite having deficits in their functional outcomes scores, limitation in their daily activities and development of adjacent joint degeneration [49,50]. The functional and clinical significance of ipsilateral adjacent joint degeneration after ankle arthrodesis has not been fully delineated, but it is universally seen in long term follow up studies [49-51]. Despite concerns over the longterm effects of ankle arthrodesis on adjacent joint degeneration, it remains the gold standard for treatment of end-stage ankle arthritis.
The first ankle arthroplasty procedures were performed in the 1970s. Results with first generation implants were largely disappointing, and arthroplasty was for many years abandoned in favor of arthrodesis [52]. Concerns about the long term functional outcomes of ankle arthrodesis [49,50], combined with growing evidence of long term success with hip and knee arthroplasty have resulted in a renewed interest in an equivalent procedure for the ankle [53,54]. In recent years, advances in implant designs, instrumentation, and surgical technique have yielded better intermediate and long-term outcomes with total ankle arthroplasty. This has led to an increasing incidence of arthroplasty procedures in North America during the past two decades [54,55] (Figure 2).
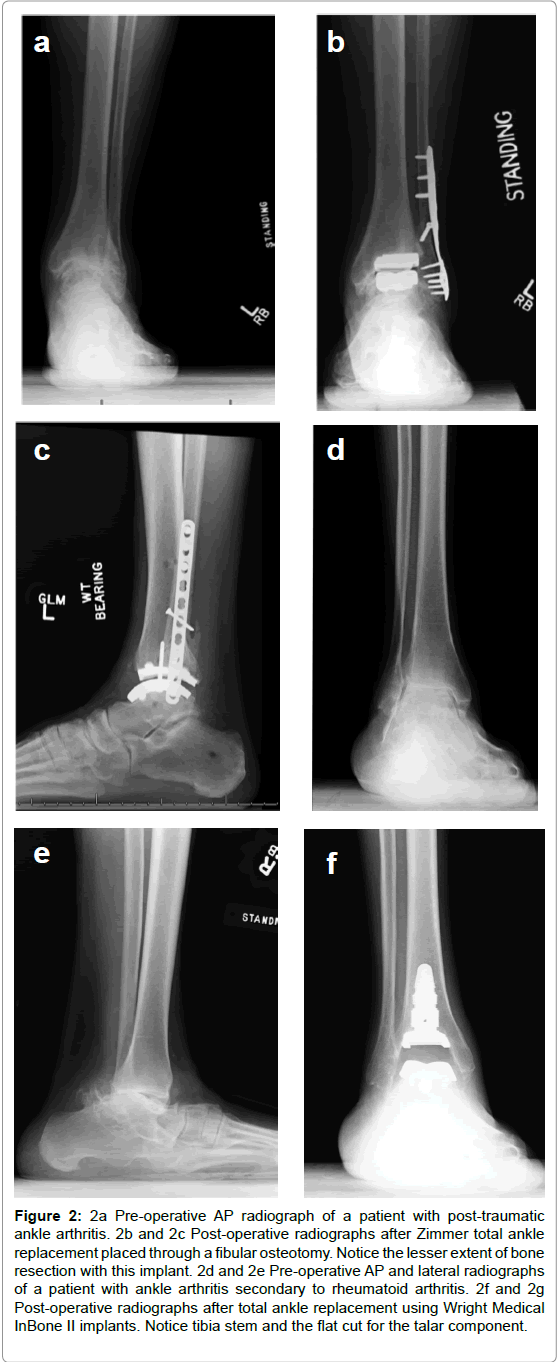
Figure 2: 2: 2a Pre-operative AP radiograph of a patient with post-traumatic ankle arthritis. 2b and 2c Post-operative radiographs after Zimmer total ankle replacement placed through a fibular osteotomy. Notice the lesser extent of bone resection with this implant. 2d and 2e Pre-operative AP and lateral radiographs of a patient with ankle arthritis secondary to rheumatoid arthritis. 2f and 2g Post-operative radiographs after total ankle replacement using Wright Medical InBone II implants. Notice tibia stem and the flat cut for the talar component.
During the early years of ankle arthroplasty, flawed implant design, instrumentation, and surgical technique resulted in a failure rates greater than 50% at 10years [48,56]. First generation implants consisted of cemented all polyethelene tibial components, and was generally of a semi-constrained design. The evolution of the modern implant saw the introduction of metal tibial component with either a fixed or mobile bearing, commonly referred to as two component or three component designs. Both two and three components implants are widely used within the U.S., but most of the literature to date concerning long-term outcomes of total ankle arthroplasty is non-comparative and does not support one implant design over the other.
Quality studies of intermediate and long-term outcomes of total ankle arthroplasty are sparse; however, the overall trend points towards improved implant survival and equivalent functional outcomes when compared to ankle arthrodesis. In a systematic review of the ankle arthroplasty literature, Gougoulias et al. identified thirteen level IV studies with a minimum of twenty patients and follow up greater than 2 years. Implant design was mixed between modern two and three component designs. In his review, patients were found to have improved clinical outcome scores and modest improvements in ankle range of motion, but residual pain was frequent (23-60%) and the overall failure rate was 10% (range 0-32%) at 5 years [57].
Haddad et al published a systematic review of intermediate and long-term results of ankle arthroplasty and ankle arthrodesis. Their review included 10 studies with 852 ankle arthroplasties and 39 studies with 1262 ankle arthrodesis procedures. Mean AOFAS scores were not significantly different among procedures. Arthroplasty implant survival rate was 78% at 5 years and 77% at 10 years. The revision rate following arthroplasty was 7%, with the primary reason for revision being loosening and/or subsidence. In the arthrodesis group, the revision rate was 9% with main reason for revision being nonunion (65%) [58].
Several authors have used gait analysis in an effort to objectify the differences between ankle arthrodesis and arthroplasty patients. Flavin et al compared gait analysis of 14 total ankle arthroplasties and 14 ankle arthrodesis patients with 14 normal controls. In their study, arthroplasty patients were found to have a significant increase in dorsiflexion, and ankle fusion patients had a significant increase in plantar flexion range of motion. Total sagittal motion, however, was not significantly different between the two groups. Both the ankle arthrodesis and ankle arthroplasty patients had significant improvement from their preoperative function, but neither group functioned as well as the normal controls. They concluded that major parameters of gait were comparable after non-deformed ankle arthroplasty and deformed ankle arthrodesis [43]. In a gait study by Singer et al it was noted that arthroplasty patients had a greater sagittal range of motion than arthrodesis patient, but neither group was using normal plantar flexion strength or motion. Nonetheless, arthroplasty patients had a gait pattern more closely resembling normal controls when compared to the arthrodesis group. They attributed this difference to an increase in dorsiflexion in the arthroplasty group compared to the arthrodesis group (11.9 vs. 6.8). Both patient groups had similar improvements in self-reported clinical outcomes scores [59].
Despite significant improvements in ankle arthroplasty, complication and failures are still relatively common compared to ankle arthrodesis, and long-term outcome and survival data is lacking. Nonetheless, the undesirable effects of ankle arthrodesis on adjacent joints, combined with our patients desire to maintain ankle motion and a more normal gait pattern have pushed ankle arthroplasty to the forefront. Indications for total ankle arthroplasty remain the subject of considerable debate in the orthopaedic community. In general, the same principals applied to patient selection for hip and knee arthroplasty should also be applied to patients desiring total ankle arthroplasty. We recommend arthroplasty for older, low demand patients wishing to maintain motion at the ankle joint. We also have a preference for ankle arthroplasty in patients with pre-existing hindfoot or midfoot arthritis. Generally accepted contraindications for total ankle replacement include: active or recent infection, Charcot arthropathy, avascular necrosis of the talus, severe deformity, vascular impairment, a compromised soft tissue envelope, severe ankle instability, and neurologic dysfunction of the limb.
Ankle arthritis can be a debilitating condition for many patients. Initial treatment options for patients presenting with symptomatic ankle arthritis include: anti-inflammatory medication, injections, and bracing. Patients who fail to respond to these treatment strategies will often benefit from surgery in the form of ankle arthrodesis vs. total ankle replacement. Ankle arthrodesis has been the mainstay of operative treatment for ankle arthritis; however, advances in ankle arthroplasty have resulted in improved short-term and mid-term outcomes leading to a trend toward increasing numbers of total ankle arthroplasties performed in recent years.
