Review Article - (2015) Volume 4, Issue 4
Objective: To show the contribution of antiphosphatidylethanolamine antibodies (aPE) screening in Antiphospholipid antibody syndrome (APS) diagnosis, especially in Antiphosphopholipid Syndrome (SNAPS) patients, based on litterature data.
Methods: A comprehensive literature review of English-language articles from January 1st 2000 to December 31th 2014 was performed using PudMed. Keywords used for the search were: seronegative antiphospholipid antibody OR phosphatidylethanolamine function, biosynthesis and physiological roles OR antiphosphatidylethanolamine antibody OR seronegative antiphospholipid syndrome.
Results: Although aPE was not included in the Sapporo criteria for the classification of APS, many studies described a significant association between aPE and the main clinical events of APS: thrombosis and obstetrical complications.
Conclusion: Because of aPL family’s heterogeneity, it appears necessary to look for non-criteria aPL in order to improve the diagnostic yield in APS, especially in patients with SNAPS. One of the most promising of this heterogeneous aPL family is aPE. Although these molecules may allow early detection of APS, their clinical relevance is still debatable and needs standardized aPE ELISA, in addition to well-designed clinical studies to confirm its diagnostic value, such as the association between recursion of thrombotic events and the presence of aPE.
Keywords: Seronegative antiphospholipid antibody; Phosphatidylethanolamine function; Biosynthesis and Physiological roles; Antiphosphatidylethanolamine antibody; Seronegative antiphospholipid syndrome
APS is an acquired prothrombotic disorder of young adults diagnosed by the presence of at least one of the two major clinical manifestations (venous and/or arterial thrombosis [1] and/or obstetric morbidity [2]) of the syndrome in combination with the persistence (for > 12 weeks) of high titers of aPL, as IgG or IgM aβ2GPI or aCL detected by enzyme linked immunosorbent assay (ELISA), or LA [3]. These conventional markers [4] should be investigated in patients with evocative clinical events of APS.
Nevertheless, it is possible to find patients with discrepancies between antibody levels and clinical disease expression. As for lupus or rheumatoid arthritis, the concept of SNAPS was mentioned for the first time in 2003 by Hughes and Khamashta [5]. The diagnosis of SNAPS has been suggested for patients presenting clinical manifestations highly suggestive of APS but persistently negative for conventional markers. Like classical APS, SNAPS patients can present an accelerated progression of disease resulting in multi-organ thrombosis.
To improve the diagnosis and thus the management of SNAPS patients, other antigenic targets have been proposed in the literature. Among them, a zwitterionic phospholipid, PE has been described as an antigenic target of “unconventional” antiphospholipid antibodies. Although autoantibodies directed against PE have not been included in APS criteria [6], they have been described as correlating with main clinical manifestations of APS.
In this review, biosynthesis and physiological roles, in particular in coagulation, of the PE will be exposed. The goal is to better understand the pathological hypothesis proposed for autoantibodies directed against PE associated with thrombosis or obstetric morbidity, the, main major clinical manifestations of APS.
Antigenic Target: Pe
In this first part, we are primarily interested in the chemical structure of PE, the different ways of its biosynthesis and in its implications in the coagulation system.
PE Structure
PE is a dominant aminophospholipid in most living organisms [7], which is asymmetrically distributed in the biological membrane [8], and mainly located, in the inner leaflet [8-11]. PE represents 25% of mammalian phospholipids and is particularly enriched in the brain [12] (45% of total phospholipids) (Figure 1). In membranes, PE exists in two conformations. It is usually in a lamellar phase, but it can also adopt a hexagonal phase [13]. There are two types of hexagonal phases: phase I (HexIPE) if the polar heads of the phospholipids are turned outwardly of the cylinder and phase II (HexIIPE) if turned in wardly of cylinder. PE can pass from the phase I to II, depending on the cholesterol content and the ionic environment and protein. Hex II PE appears to be more immunogenic than Hex I PE, and the presence of PE in this configuration may facilitate the formation of autoantibodies directed against PE, or the interaction of PE with LA.

Figure 1: The phosphatidylethanolamine structure. This neutral phospholipid is formed by a combination of a residue phosphoethanolamine and a glycerol residue esterified with two fatty acids (R1 and R2).
Biosynthetic pathways
There are four biosynthetic pathways for PE synthesis in mammalian cells: the phosphatidylserine decarboxylation (PSD) pathway, the CDP-ethanolamine (CDP-etn) pathway, the acylation of lyso-PE by lyso-PE acyltransferase [14,15] and the production in the endoplasmic reticulum by a calcium-dependent base-exchange reaction [16,17] (Figure 2).

Figure 1: Biosynthesis of phosphatidylethanolamine. There are two quantitatively major pathways for PE synthesis in mammalian cells: the phosphatidylserine decarboxylation (PSD) pathway and the CDP-ethanolamine (CDP-etn) pathway. In the latter, ethanolamine (etn) is phosphorylated by ethanolamine kinase (EK) to produce phosphoethanolamine which is converted into CDP-ethanolamine by CTP:phosphoethanolamine cytidylyl transferase (ET). In the final reaction of this pathway, CDP- ethanolamine:1,2- diacylglycerol ethanolamine phosphotransferase (EPT) combines diacylglycerol with CDP-ethanolamine to produce PE. Besides these two main pathways, there are two other minor biosynthetic pathways: the acylation of lyso-PE by lyso-PE acyltransferase and also by a base-exchange reaction in which PS is converted to PE by the exchange of serine in PS for ethanolamine by the action of PS synthase-2.
Functions
PE participates in multiple facets of cell biology, exerting a pivotal role in cellular processes [12], such as membrane fusion/fission [18,19], cell cycle regulation [7], apoptosis, and more recently, autophagy [20,21].
In addition to contributing to membrane structure, PE is involved in the fundamental process of coagulation. Although phosphatidylserine is the preferred phospholipid for all of the coagulation complexes [22], several studies report the essential role of PE as a cofactor for the anticoagulant activity of activated protein C (APC) [23]. These studies demonstrate that when PE is added to liposomes already containing an optimal concentration of phosphatidylserine, proteolytic inactivation of factor Va by APC is greatly improved in a concentration-dependent manner [24,25]. However, the rate of factor Va inactivation observed in the presence of PE could not be achieved with any concentration of phosphatidylserine, indicating that PE contributed to the reaction which cannot be substituted for by additional phosphatidylserine [23,25].It was also proposed that polyinsaturation of the fatty acid chains of PE [26] and the oxidation of PE containing vesicles were also able to enhance APC anticoagulant activity, almost doubling the clotting time, and no such effect was observed if the vesicles were devoid of PE [23]. It was subsequently shown that the structural basis of PE-dependent APC ctivity was localised on the protein C Gla domain because its substitution abolishes the PE-dependent proteolytic activities. Gla domain confers a binding specificity toward PE, and allows a synergistic interaction with factor Va and phosphatidylserine on PE-containing membranes [25,26]. Additional experimental data demonstrate that PE is an inhibitor of the factor Xaprothrombin system [27], and that the addition of phosphatidylserine and PE into the same liposome surface caused synergy in promoting heparin's anticoagulant effect [28].
Moreover, procoagulant properties of PE have also been described. PE facilitates tenase complex formation (an enzymatic complex composed of the serine protease, factor IXa, a protein cofactor, factor VIIIa, a phospholipid membrane, and Ca2+) which enhances factor Xa generation [29]. In the same way, PE was identified as a phospholipid- associated VLDL responsible for the stimulation of the lipoprotein of the contact pathway [30].
Pathological Hypothesis of aPE
Since the 90s, the antiphosphatidylethanolamine antibodies (aPE) have been described in the literature as associated to procoagulant properties and several mechanisms have been proposed to understand the involvement of antiphosphatidylethanolamine antibodies in the pathophysiology of antiphospholipid syndrome.
Inhibition of APC’s activity
It has already been shown that the anticoagulant activity of APC was enhanced by PE, or, to a lesser extent cardiolipin [22-24]. These two phospholipids are major targetsofAPS [31-33] and PE constitutes a more important component of the APC anticoagulant complex than of the procoagulant complexes [33]. As previously described, PE are mainly located in the inner leaflet of biological membranes, so it is possible that a primary event in APS patients exposes PE molecules in the outer part of the membrane, making possible the binding of aPE [34]. Recent experiments utilizing rat aortic arch showed high levels of PE distributed at the blood–endothelium interface, where PE presents a potential vulnerability to aPE autoimmunity and supports an underlying immunological cause for aPE-associated thrombotic risks [9]. In a reconstituted coagulation system with PE-containing membranes, aPE isolated from patients with idiopathic arterial and/or venous thrombosis potently inhibits the APC anticoagulant activities [24,25]. These observations are in keeping with the notion that aPEpositive autoimmune disorders likely result in the masking of endothelial PE, whereby it impedes its participation in anticoagulation pathways at the vascular luminal surface. Such interference may shift the coagulation potential sufficiently to promote a greater thrombotic risk [9], similar to that observed with patients with decreased protein C level [35,36]. In conclusion, aPE may be responsible fora form of acquired resistance to protein C dependant phospholipid (Figure 3).
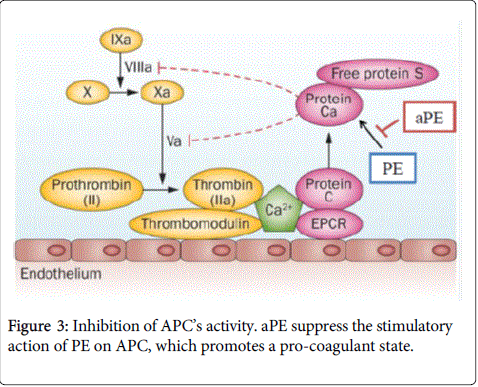
Figure 3: Inhibition of APC’s activity. aPE suppress the stimulatory action of PE on APC, which promotes a pro-coagulant state.
Antibodies to PE-binding plasma proteins
We recently reported that certain aPE are not specific for PE, but are directed to PE-binding plasma proteins involved in the coagulation cascade, such as high-molecular-weight kininogen (HK), lowmolecular- weight kininogen (LK), proteins in complex with HK, factor XI, or prekallikrein [38]. Recently, prothrombin has been added to this list [10]. Moreover, PE was found to induce specific conformational changes in the kininogens recognizable by aPE [38,39] and autoantibodies to kininogen-PE complexes enhanced thrombininduced platelet aggregation [40]. In obstetric APS, disruption of the kallikrein–kinin system by aPE antibodies might play a pathogenic role in early pregnancy losses [41].
Relationship with LA
Other studies have also described an interaction between PE and lupus anticoagulant (LA). for the first time a case of primary APS whereby a LA was accompanied only by an IgM aPE [42].
In 1993, it was described that plasma reactivity to He II PE was more frequently associated with LA than with aPE [13]. Indeed, it has been demonstrated that Hex II PE is immunogenic in mice and has been used in a new clotting assay to detect lupus anticoagulant [43]. The potential specificity of LA for PE has been validated in a study in which human monoclonal antibodies were prepared from the lymphocytes of a patient, and these antibodies all exhibited a high degree of specificity toward PE, especially in the hexagonal phase [44]. Due to the ability of the hexagonal phase PE to inhibit the prolongation of the clotting time, several groups suggested that LA might represent a subset of aPE [34,38].
Autoantibodies: aPE
Although aPE was not included in the Sapporo criteria for the classification of APS [6], many studies described a significant association between aPE and the main clinical events of APS: thrombosis and obstetrical complications.
aPE detection method
A little variability in the method of aPE detection is reported in the literature because methods are generally derived from ELISA method described by Sanmarco and et al. [39].
Clinical associations
Thrombosis
In 1996 Berard and al. [45] reported a case of a patient with thrombosis and cutaneous disease. In 2002, among 20 cases of patients potentially related to APS, 17 were aPE with only 10patients presenting arterial thrombosis and 9 venous thrombosis (5 had both) [46].
In 2005, Kalashnikova and al. [47] described the prevalence and clinical significance of IgG aPE in 28 patients with Sneddon’s syndrome (cerebrovascular disturbances and extensive livedo reticularis). To do this, they measured aPE and classic immunological APS markers (aCL and LA). The results showed that aPE are often (in 46% of cases) found in aCL and LA negative patients with Sneddon’s syndrome. More recently, Hasegawa and al described in 2012 two cases of livedo vasculopathy with IgG aPE and IgA aCL [48].
Two large studies have examined the association between aPE and thrombosis. In 2001, Sanmarco et al [49] have assessed the interest of aPE in unexplained thrombosis (UT, thrombotic episode without any of the main autoimmune and hereditary thrombophilic defects). They compared result from UT to patients without thrombosis but with SLE or infectious diseases (who serve as controls). A significant prevalence of aPE (18%) was seen in patients with UT in comparison to controls. In 2007 [50], a was set up to evaluate the prevalence, clinical and biological significance of aPE in thrombotic patients with or without the main known clinical and biological risk factors for . aPE and were measured in 271 patients with (234 venous and 37 arterial) and 236 matched controls. aPE were the aPL with the highest odds ratio for thrombosis ( [OR]: 4.2, p < 0.001),with no predominant isotype, no association with the main known clinical or biological risk factors for neither with a type of , arterial or venous. Of major interest, 63% of 40 aPE-positive patients were negative for the APS laboratory criteria.
Obstetric complications
To date, the most important study reporting the association between obstetric complications and the presence of aPE is that of Gris et al [51] in 2000. They conducted a hospital-based case control study on with no antecedent of thromboembolic or autoimmune disease. In this large cohort of 1554 women, they studied 3 groups of 518 : patients with early recurrent pregnancy loss (RLP), patients with explained episodes and mothers with no previous obstetrical accident. Interestingly, they reported that aPE was highly associated with unexplained recurrent early fetal loss and that aPE was the only antibody in 73% of aPL positive patients. These results are in agreement with those reported in the retrospective study of Sugi et al. [52] performed in 139 patients with unexplained RLP. Two hundred age-matched, healthy, non-pregnant female volunteers with no history of miscarriage were tested as controls. To summarize, 44 (31.7%) of the 139 patients with RPL were positive for aPE, and a positive test result for aPE was more frequent in the patients with RPL than in the members of the control group (P=.0002). Conversely, there was no statistically significant difference in the incidence of positive test results for other aPL between the RPL group and the control group. in 2010, Obayashi et al. [53] reported prevalence of aPE is higher in RPL patients than in women with normal pregnancy, aPE elevation is not an independent risk factor to predict further miscarriage in women with two or more unexplained consecutive pregnancy losses. Positivity of aPE was also described in in vitro fertilization (IVF) outcome. In 2007, a prospective study [54] examined the of aPL in 101 who had undergone IVF and the relationship between aPL and IVF outcome. This prospective study shows that aPE were the most prevalent aPL in infertile but do not support an association between aPL and IVF outcome.
This relationship with obstetric complication was confirmed in the literature by two studies in mice. First, in genetic knockout studies where a deficiency in ethanolamine kinase 2 (enzyme which catalyzed the first step in the CDP-ethanolamine pathway) results in placental thrombosis and spontaneous fetal death [55].Then, in a second study where mice passively immunized with aPE showed impairment of trophoblast giant cell invasion and increased placental, apoptosis, thrombocytopenia, increased fetal resorption and thrombosis in the placenta, features close to the human APS [56]. Moreover, it would appear that aPE and aPS are associated with increased natural killer cell activity in non-male factor infertility patients [57].
aPE and SNAPS
Some authors are skeptical about the diagnosis of SNAPS [58-60], making the classification of these patients controversial. Three main explanations for the existence of SNAPS have been proposed: first, the diagnosis may be wrong, second previously positive aPL tests have become negative and third most likely, conventional testing failing to pick up cases with antibodies directed against different phospholipids or protein cofactors [5].
Indeed, aPL represent a heterogeneous family of antibodies reacting with phospholipid-binding plasma proteins (prothrombin, protein C, protein S, annexin V and domain I of β2GPI), phospholipid protein complexes (vimentin/cardiolipin complex) and anionic phospholipids other than cardiolipin (phosphatidic acid , phosphatidylserine and phosphatidylinositol) [61,62]. So, one of the most critical issues is that the currently available assays cannot detect all potential aPL, and the new specificities, recently identified, are tested in only a few research laboratories. Another important issue is transient aPL seronegativity which may be due to different causes, such as nephrotic syndrome, treatment with corticosteroids, immunosuppressants, or antibody consumption during thrombotic event [46].
Few articles in the literature [63] described obstetric complications in SNAPS with only positive aPE, but in 2003, Pourrat and al. reported the case of a patient of 38 years who presented a miscarriage at 8SA with only IgG aPE [64]. In the same way, in 2009, Sanmarco and al [65] described aPE detected in the absence of other aPL since 60% of aPE positive sera were SNAPS patients, underscoring the importance of detectingthese antibodies in these patients.
The mechanisms by which aPL cause thrombosis and obstetric morbidity are poorly understood, but probably include inhibition of natural anticoagulants, activation of platelets and endothelial cells, blocking of the fibrinolytic system, and triggering of the complement cascade [66]. A ‘second hit’, frequently linked to innate inflammatory responses, and is probably necessary to initiate the thrombotic vasculopathy characteristic of APS [67].Evidence shows that the dominant antigenic targets for aPL in APS are phospholipid-binding plasma proteins such as β2GPI [68].
Because of aPL family’s heterogeneity, it appears necessary to look for non-criteria aPL in order to improve the diagnostic yield in APS, . One of the most promising members of this heterogeneous aPL family is aPE. Indeed, some studies have reported that aPE could be the only aPL present in patients with UT or in patients with SNAPS.
PE plays a fundamental role in the structure of cell membranes and is involved in many cellular processes, such as membrane fusion/ fission [18,19] or cell cycle regulation [20], in apoptosis and autophagy [21,22]. In hemostasis and coagulation system, PE appears as a major anticoagulant since it is essential to APC’s activity. So, the main candidate mechanism that has been proposed to explain the thrombotic tendencies in patients with aPE involves inhibition of the protein C anticoagulant pathway.
As with the “double hit” theory applied to β2GPI, it is possible that a primary event in APS patients expose PE molecules in the outer part of the membrane, making possible for the antibody to bind.
We previously mentioned that PE was involved in the process of autophagy, since it is coupled with the Atg8 protein [21,22]. mTOR signaling has a pivotal role in regulating autophagy, and adaptive immune responses because when activated, mTOR pathway inhibits autophagy, but its inactivation is used to remove the inhibition and thus initiate autophagy.
Recently, a study [69] has suggested that the PE binding protein 1 was involved in vascular endothelial cell autophagy and atherosclerosis; and another study showed that there was an inhibition of the mTOR pathway in APS [70], and so that the mTOR pathway was involved in the vascular lesions associated with APS. In view of these two new data, we can hypothesize that there is a relation between mTOR pathway, PE and autophagy, or even that the inhibition of the mTOR pathway may be linked to aPE.
In the same way, since it has been recently reported that certain aPE, are not specific for PE, but are directed to PE-binding plasma proteins involved in the coagulation cascade [38], we also can think that there may be other PE-binding plasma proteins not yet identified that could participate in the pathogenesis of aPE
Although aPE may allow early detection of APS, their clinical relevance is still debatable and needs standardized aPE ELISA, in addition to well-designed clinical studies to confirm its diagnostic value, such as the association between recursion of thrombotic events and the presence of aPE.
