Research Article - (2015) Volume 0, Issue 0
Introduction/objectives: Rheumatoid arthritis (RA) is associated with decreased bone mass and increased risk of fractures. However, mechanisms underlying this association are not fully understood. Thus, we quantified serum levels of sclerostin, a glycoprotein that inhibits bone formation, and determined its association with bone mineral density (BMD) and disease progression in RA patients.
Method: Forty-eight women (aged 25-83 years) with RA and 15 healthy women (aged-matched) were recruited to determine the association between serum sclerostin and BMD at femoral and vertebral level (L1-L4), by DEXA, body mass index (BMI), disease duration, disease activity score (DAS 28), C-Reactive protein and rheumatoid factor. Spearman correlation analyses were performed to determine the association between sclerostin and BMD and the additional variables listed above. A multivariate analysis was used to adjust for confounders.
Results: Serum sclerostin was not significantly different between RA patients and controls (22.59 ± 2.13 vs 19.49 ± 3.1 pmol/L). A positive correlation was found between serum sclerostin and femoral BMD (r=0.343, P=0.017), but not BMD at vertebral level. Using a multivariate analysis, the positive correlation was conserved between serum sclerostin and femoral BMD (P=0.002). There was not a significant association between sclerostin and the other variables studied.
Conclusions: While serum sclerostin levels were not significantly different between RA patients and controls, this study showed a positive correlation between serum sclerostin and femoral BMD in a small Mexican sample of women with RA. Further studies are needed to evaluate whether serum sclerostin is associated with risk of fracture in RA patients.
Keywords: clerostin; Rheumatoid arthritis; Bone mineral density; Women
Rheumatoid arthritis (RA) is an autoimmune disease affecting approximately 1% of the population worldwide [1]. RA is characterized by chronic and symmetric inflammation of synovial joints; leading to joint destruction, chronic pain, loss of function and disability [2]. Studies have shown that RA may also result in bone complications such as periarticular bone loss, bone erosions and generalized osteoporosis [3-5]. RA is highly associated with significant bone mineral density (BMD) loss in the femoral neck, lumbar spine and generalized osteoporosis and increased risk of fractures [6-9]. Indeed, the prevalence of osteoporosis in RA patients is two-fold higher in women with RA compared to subjects without RA [9]. Although osteoporosis and fractures associated with RA may lead to increased health costs, higher rates of disability and mortality, and decreased quality of life [9,10], mechanisms underlying loss of bone mass and increased susceptibility to fractures in RA are not completely understood.
Multiple factors have been suggested to be involved in the higher prevalence of osteoporosis in RA patients, such us high-disease activity (inflammation), immobility, chronic treatment with glucocorticoids (GCs) [11], as well as inherent risk factors for osteoporosis (e.g. aging and female gender) [12]. Recent animal and human studies suggest that sclerostin may affect bone remodeling in normal and pathological stages [13,14]. Sclerostin, the glycoprotein product of the SOST gene, is highly expressed in embedding bone cells such as osteocytes, chondrocytes and cementocytes [15-17]. This protein potently inhibits the Wnt/β-catenin canonical signaling pathway by binding to the low density lipoprotein receptor-related proteins L5/6, leading to decreased osteoblastogenesis and osteoblast activity, and thereby decreasing bone formation [18,19]. Several clinical studies have shown a significant increase of serum sclerostin levels with age [14,20-22] and after menopause [21-23], suggesting that serum sclerostin may be associated with aging- and menopause-induced bone loss [14,21,22]. Furthermore given that RA is characterized by a significant local and generalized bone loss [3-6], a plausible mechanism behind increased BMD loss in RA suggests that sclerostin serum levels are significantly increased and are inversely associated to BMD in RA patients. Thus, the aims of this study were to compare levels of serum sclerostin in RA patients and healthy controls and, additionally, to investigate the association between serum sclerostin and BMD in both femurs, at vertebral level (L1-L4), and disease progression in RA states.
The patients were enrolled at the Rheumatology Department of the Hospital Juarez de Mexico (Mexico City, Mexico). The recruitment occurred from March to September 2014. General information such as demographic characteristics (age, weight, height, BMI) was collected directly from all sixty-three female study patients through a questionnaire. Additionally, data collected from patients in the RA group included current treatment and medication information, and, severity and duration of disease.
Exclusion criteria for the RA group consisted of patients diagnosed with fibrous dysplasia, sclerosteosis and Van Buchem disease; use of contraceptives, post-menopausal women with hormone replacement therapy, chronic alcoholism and smoking habits. Additionally, patients with a history of fragility fracture in the last 2 years were excluded from the present study. After application of the exclusion criteria, the RA group included 48 women from 25-83 years of age. Fifteen age-matched women without diagnosis of RA or osteoarthritis (nurses, medical residents from the same Hospital) were included as the control group. All subjects gave written informed consent for participation in the study, and each subject was adequately informed about the research procedure and the main goal of the study. The Hospital Juarez de Mexico ethics committee approved this project.
Diagnosis of RA
All 48 women were diagnosed with RA for the Rheumatology Department according to the American Rheumatism Association Criteria [24]. Accordingly, all patients showed significant disease activity assessed by high-sensitivity C-reactive protein (hsCRP), erythrocyte sedimentation rate (ESR), positive rheumatoid factor (RF) and disease activity score of 28 (DAS 28). The DAS28 is a measure of disease activity in RA and is based on a count of 28 swollen and tender joints, with a score ranging from 0 to 9.4. The DAS28 is widely used to objectively evaluate a patient’s response to treatment [25].
In the present study the primary condition used for inclusion was positive rheumatoid factor and, as our population was under treatment, a minimum DAS score accepted was ≥ 2.6.
Laboratory methods
After fasting for at least 12 hours, blood samples were collected from both patient and control groups. Venous blood was collected from the right arm by antecubital venepuncture. Two blood samples were anticoagulated in EDTA for erythrocyte sedimentation rate and hematological analysis. Complete blood count (hemoglobin, hematocrit and platelet count) and differential count parameters (leukocytes, neutrophils and lymphocyte count) were measured with a high-volume hematology analyzer (ADVIA® 2120i hematology analyzer system, Siemens). For analysis of serum, samples were collected in regular laboratory serum tubes. The samples were centrifuged at 1980 g for 20 min and the serum was decanted and stored at -80 degrees until the assessment of inflammation markers could be performed. C-reactive protein was determined using a commercially available kit (CRP latex, cat. 72100280, BIO-RAD), and the reumaclin kit, (cat. 72130180, BIO-RAD) was used to determine the rheumatoid factor. The detection limit of each assay was: 6 mg/dL and 3 UI/L, respectively.
Determination of serum sclerostin
Serum sclerostin levels were measured using commercially available enzyme linked immunosorbent assay (ELISA) kits [14,21]. Assay was performed using polyclonal goat anti-human sclerostin antibody as a capture antibody, and biotin-labeled mouse monoclonal anti-sclerostin as a detecting antibody. The standard curve was read between 0 and 240 pmol/l with a detection limit of 2.6 pmol/l. The parameters of coefficient variation were ≤ 7 and ≤ 10 for intra-assay and inter-assay precision respectively. All samples were run, simultaneously, in duplicate.
Determination of BMD
To determine BMD at the lumbar spine (anteroposterior projection of L1-L4), right and left proximal femurs (middle-diaphysis), and the patients were assessed using central dual-energy X-ray absorptiometry (DEXA; GE lunar Prodigy densitometer, GE Medical Systems; software version 8.8). The BMD data are presented in g/cm2. The same technician performed all BMD measurements.
The quantitative variables were expressed as the mean +/- SEM., and the comparisons were measured using analysis of variance (ANOVA) followed by Bonferroni post hoc correction. When comparing two groups, Student t test for parametric data and Mann-Whitney U test was applied for non-parametric data. Spearman correlation coefficient was used to evaluate the strength of association between BMD and other clinical variables that failed the normality test. A multiple regression analysis (stepwise method) was used to adjust for confounders. In the final model, the dependent variable was BMD at vertebral level, and right and left femurs. Statistical significance was considered as p< 0.05. All statistical analyses were performed using GraphPad Prism software V5 (GraphPad Software, Inc., San Diego, CA. USA) and SigmaPlot software V12.0, (SYSTAT, Software Inc., San Jose, CA. USA).
Characteristics of the study populations
In the present study, the RA group included a total of 48 patients that met the inclusion criteria and 15 age-matched healthy women as the control group. The results show no statistically significant differences between the control and the RA group for the demographic data and BMD values. Moreover, the clinical parameter, ESR (a parameter of disease activity) was significantly greater in RA patients as compared to control subjects (p<0.004) and both hemoglobin concentration and percent of hematocrit were significantly lower in RA patients versus healthy women; whereas that there were no significant differences in the % of neutrophils, lymphocytes and leukocytes between RA women and control women (see Table 1).
The mean disease duration time was 8.9 years with a mean DAS score of 2.88, suggesting that RA patients have low disease activity or are in clinical remission. Likewise, most of the patients (70%) were currently under methotrexate treatment with a mean dose of 12.13 ± 0.63 mg/week (Table 2).
Serum sclerostin levels
Figure 1 shows that serum levels of sclerostin, as determined by ELISA, were not significantly different between the patients with RA and the control subjects. Additionally, when patients were divided by years of RA duration (0-5 years, 6-10 years, >11 years), the serum levels of sclerostin were not significantly different between groups (data not shown).
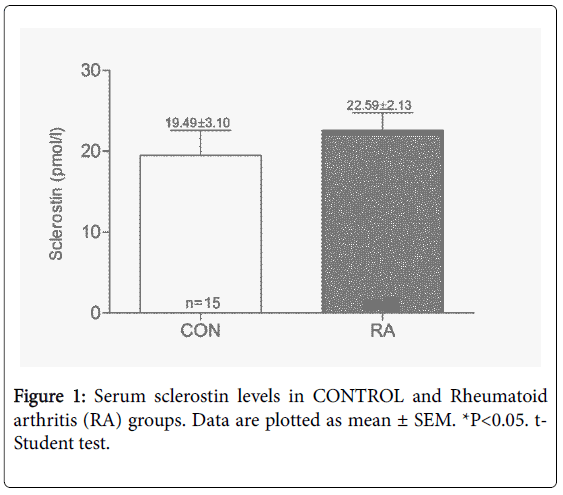
Figure 1: Serum sclerostin levels in CONTROL and Rheumatoid arthritis (RA) groups. Data are plotted as mean ± SEM. *P<0.05. t- Student test.
Determination of BMD in RA patients
The RA group was sub-divided into three groups according to the length of time since RA diagnosis, and BMD of vertebrae and both femurs was subsequently determined using DEXA. At vertebral and right femoral levels, there was a progressive BMD loss but only patients with RA for more than 11 years had a significantly lower BMD as compared to control group or patients with RA for 0-5 years (Figure 2A and 2B). The left femur results trended towards a small and progressive decrease in BMD as disease duration increased (Figure 2C).
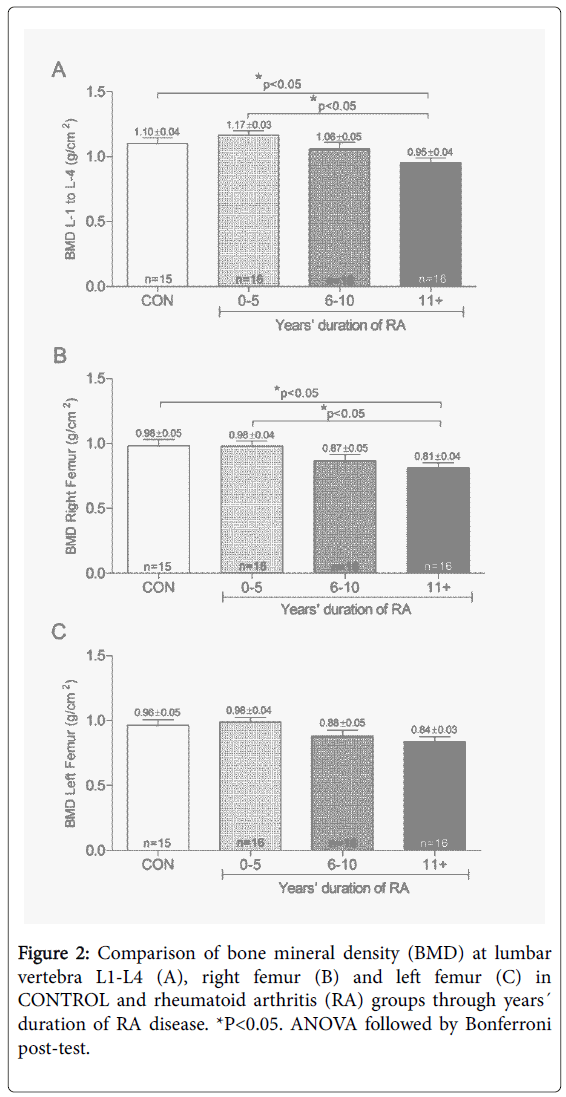
Figure 2: Comparison of bone mineral density (BMD) at lumbar vertebra L1-L4 (A), right femur (B) and left femur (C) in CONTROL and rheumatoid arthritis (RA) groups through years´ duration of RA disease. *P<0.05. ANOVA followed by Bonferroni post-test.
BMD and sclerostin in RA group
In RA patients, serum sclerostin did not positively correlate with BMD at L1-L4 level (Figure 3A), while a positive correlation was found in the right and left femur (r=0.330, p=0.02; r=0.348, p=0.015; respectively; Figure 3B and 3C). Then, a multivariate analysis was used for additional covariates (age, BMI, disease duration, DAS 28, RF, BMD mean femoral and BMD L1-L4), and the correlation between serum sclerostin and the mean femoral BMD persisted (P<0.002) (Table 3).
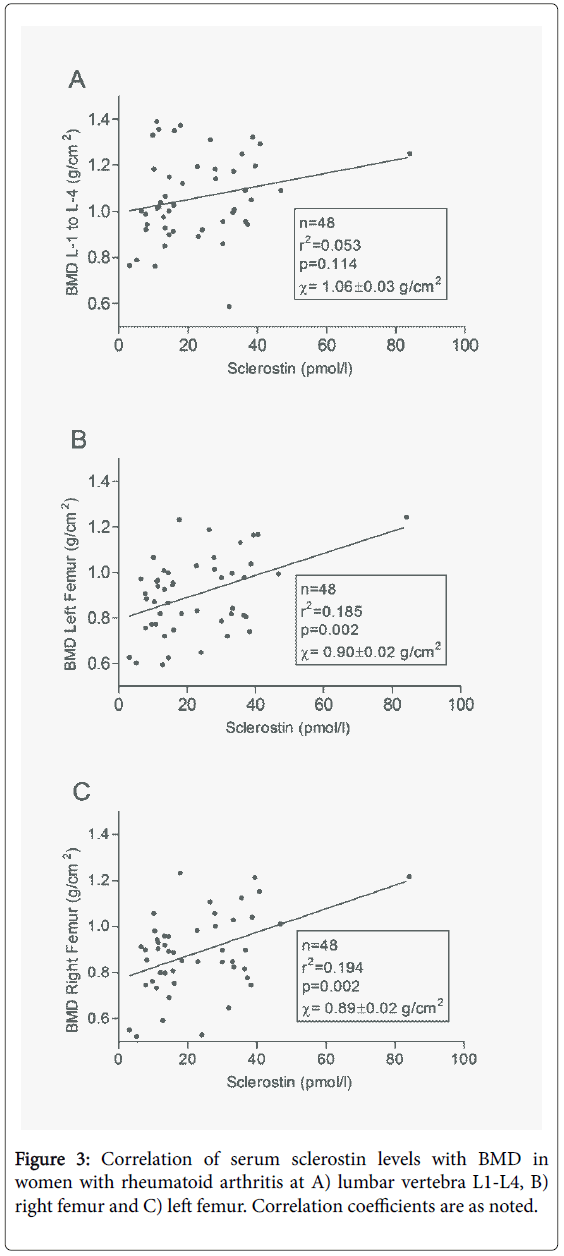
Figure 3: Correlation of serum sclerostin levels with BMD in women with rheumatoid arthritis at A) lumbar vertebra L1-L4, B) right femur and C) left femur. Correlation coefficients are as noted.
This study, performed in a Mexican sample population, shows that serum levels of sclerostin are not significantly different between women with RA and healthy women. Additionally, in women with RA there is 1) a significant loss of the BMD at L4 vertebra and femoral levels as time of disease increases, and 2) a positive correlation between serum sclerostin levels and mean femoral BMD. Sclerostin is a glycoprotein product of the SOST gene and is highly expressed in embedding bone cells such as osteocytes, chondrocytes and cementocytes [15-17]. This protein potently inhibits the Wnt/β-catenin canonical signaling pathway by binding to the low density lipoprotein receptor-related proteins L5/6, leading to decreased osteoblastogenesis and osteoblast activity, and thereby decreasing bone formation [26].
Human studies have shown a significant increase in serum sclerostin levels with age [14,20-22] and after menopause [21-23], suggesting that increased serum sclerostin may be associated with BMD loss induced by aging and menopause [14,21,22]. Furthermore, other studies [26,27], but not all [20,28], have shown that increased serum sclerostin concentrations are associated with a greater risk of suffering fracture in older postmenopausal women. On other hand, several reports have demonstrated that RA is highly associated with significant BMD loss mainly in the femoral neck and lumbar spine and greater risk of fractures in these anatomical sites [6-9,29,30]. In light of these findings, our first hypothesis was that sclerostin serum levels would be significantly increased in the RA group as compared to control group. However, in the present study, there were no significant differences between the sclerostin serum levels in RA patients when compared to the control group. Our results are in agreement with a recent study performed in a French population, in which it was demonstrated that no significant differences in serum sclerostin levels were found between French RA patients and the control group [31].
While we do not know the reasons why serum sclerostin is not increased in RA patients, we propose some potential explanations. First, it has been reported that bone specimens from patients with RA have an increased osteocyte death as reflected by an augmented number of empty lacunae as compared to bone from healthy subjects [32]. Thus, this could reduce the synthesis and release of sclerostin by osteocytes into the circulation of RA patients. Finally, in our study at the time of sclerostin determination, 50.98% of RA patients were in clinical remission (DAS score ≤ 2.6) and 72.55% were under methotrexate treatment. As sclerostin expression by osteocytes has a positive correlation with inflammation [33], it is possible to speculate that the lack of increase of serum sclerostin in RA patients may be partially due to low disease activity.
An epidemiological study has shown that patients with RA are more susceptible to suffering fractures as compared to non-RA patients, regardless of age, sex or anatomic site [12]. While our study did not determine fracture risk, we did find significant BMD loss at both vertebral and femoral levels as disease duration increases in Mexican women. This finding is in line with several studies demonstrating a progressive loss of BMD during evolution of the disease in the right femur and at the L1-L4 vertebral level [9,12].
This report shows a positive correlation between serum sclerostin levels and BMD in both right and left femur, but not at L1-L4 vertebral level. Given that patients with RA have a significantly lower BMD than healthy people, and that sclerostin is a potent inhibitor of bone formation, it was initially predicted that serum sclerostin levels would negatively correlate with BMD in patients with RA. However, the current study results showed a positive correlation between femoral BMD and serum sclerostin in patients with RA. In partial agreement with our results, it was recently demonstrated that serum sclerostin levels have a positive correlation with vertebral BMD, but not with femoral BMD [31].
The reasons behind these differences may include factors such us gender and age, as 1) sclerostin serum levels are gender- and age-dependent [2,14,20] in our study only women were included versus a study population of 74.7% of women with RA in the previous study [3,31] the mean age of our RA population was 50.81 ± 1.66 years-old versus 60.7 ± 8.5 years-old of the previous study [31]. The reasons for the paradoxically positive association between circulating sclerostin (a potent inhibitor of bone formation) levels and BMD are unknown. However, it is possible that circulating sclerostin levels may not reflect changes of sclerostin at a local level [34]. Future studies are needed to determine sclerostin levels at local sites (bone, synovium, bone marrow) and determine its association with disease progression and BMD in RA patients.
Our study has some limitations including 1) a small sample of RA patients and most of patients were under treatment with disease-modifying antirheumatic drugs, 2) most of the RA patients were at low activity of disease or disease remission. Thus, it is unclear whether sclerostin levels are increased when there is a high disease activity, 3) fracture risk was not determined in this study and 4) in this study renal function was not measured. In summary, serum sclerostin was found not to be significantly different between RA patients and healthy subjects and there is a positive correlation between serum sclerostin and femoral BMD in a small Mexican sample of women with RA.
