Research Article - (2015) Volume 4, Issue 2
Aim: Our aim is to assess comparative interleukin 4 and interleukin 13 levels in serum and in synovial fluid for patients with psoriatic and rheumatoid arthritis as well as comparative evaluation of serum levels of these antiinflammatory cytokines with lumbar T score. Methods: The study was performed on three groups: group 1 consists of 27 patients with psoriatic arthritis, group 2 consists of 21 patients with rheumatoid arthritis, and the control group consists of 20 healthy patients. For each of these groups we have identified the anti-inflammatory cytokines in blood and synovial fluid. We also established a clinically useful correlation between blood concentration of these cytokines and lumbar T score. Results: In group 1 serum IL-4 in most patients showed no detectable serum concentration, and IL- 13 had values between 2.67 and 4.99 pg/ml, p1<0.01-ES, and the lumbar T score was ranged between 1.58 and 1.77 DS, p?1<0.01. In group 2 serum IL-4 in most patients showed no detectable serum concentration, and IL-13 had values between 2.21 and 13.32 pg/ml, p2<0.002-ES, and the lumbar T score had values between -2.51 and -3.41 DS, p?2<0001-ES. In the control group IL-4 was not detected in serum, serum IL- 13 had values between 2.05 and 3.35 pg/ml, and the lumbar T score had values between 0.29 and 1.3 DS. In the synovial fluid the interleukin-4 and interleukin-13 were found in both groups of the patients studied. We also found that in patients with psoriatic arthritis there is an increase in the ratio of the concentration of IL-13 in synovial fluid and blood as opposed to those with rheumatoid arthritis. Conclusion: There are significant differences regarding the profile of anti-inflammatory cytokines from serum and synovial fluid of patients with psoriatic and rheumatoid arthritis, also in psoriatic arthritis exist a local production of interleukin-13 in the inflamed joint.
Keywords: Psoriatic arthritis; Rheumatoid arthritis; Antiinflammatory cytokines; Osteoporosis
The involvement of numerous cytokines in inflammatory disorder of the synovium affected by psoriatic arthritis creates a permanent antagonism between proinflammatory and anti-inflammatory cytokines [1,2].
The existent cooperation necessary to suppress the proinflammatory effects of natural interleukin-1 (IL-1) and tumor necrosis factor alpha (TNF-α), causes increased expression of interleukin-4 (IL-4) and interleukin (IL-13) with protective role of the inflammated synovium [3-6].
Interleukin-4 is a cytokine synthesized by CD4+ Th2 lymphocytes, being characteristic for this subset of lymphocytes. In addition to the lymphocyte, the interleukin -4 is also secreted by mast cells and basophils [7-10].
The results of the comparative study on the role of interleukin-4 in the occurrence of psoriatic arthritis and arthritis have shown that this cytokine can cause, besides the anti-inflammatory action, an inhibitory action of the synoviocytes proliferation, reducing collagenase synthesis and augmentation of IL-1Ra synthesis of the synoviocytes [4,6].
The comparative determination for the concentration of interleukin-4 and interleukin-13 of synovial fluid in psoriatic arthritis and rheumatoid arthritis revealed the presence in both diseases of these inflammatory cytokines, but in psoriatic arthritis their level is much lower than in rheumatoid arthritis [11].
The Interleukin-13 has “IL-4” functions, but less intense. The source of interleukin-13 is the LTCD4 + (Th0, Th1 and Th2) and LTCD8 [12].
The interleukin 13 has an inhibitory activity on the mononuclear/ macrophage system, and also stimulating activity of this system function. Thus, the interleukin-13 inhibits the synthesis of proinflammatory cytokines IL-1, IL-1, IL-6, TNF-α, IFN-d, as well as the level of chemokine (IL-8).
Some comparative studies regarding the level of interleukin-13 in synovial fluid and blood of the patients with psoriatic arthritis were made recently. The result of these studies, show that the synovial fluid interleukin- 13 concentration was significantly higher in patients with psoriatic arthritis than in those with other types of arthritis, including rheumatoid arthritis [13].
Regarding the serum concentration of the interleukin-13 in patients with psoriatic arthritis, it was lower than in patients with rheumatoid arthritis. It was also observed that all patients with psoriatic arthritis had higher concentrations of interleukin-13 in synovial fluid than in peripheral blood [13].
The ratio of interleukin-13 concentration in the synovial fluid and peripheral blood was higher in patients with psoriatic arthritis than in patients with rheumatoid arthritis. From these studies it can be concluded, that in psoriatic arthritis seems to be a local production of IL-13 in the affected joint [13].
The purpose of the study
The production and biological activities of anti-inflammatory cytokines have been studied in psoriatic arthritis and in particular in animal models. The extrapolation of the results obtained in these studies in humans is not always sufficient and real. In the literature there are relatively few studies that evaluate in vivo, for blood and synovial fluid the inflammatory cytokines.
These findings led to the personal interest to study antiinflammatory cytokines in psoriatic arthritis as well to evaluate the correlation between these cytokines and proinflammatory ones on the one hand, and bone mineral density, on the other hand.
The purpose of this study is the comparative evaluation of the interleukin 4 and interleukin 13 level in serum and synovial fluid at patients with psoriatic arthritis and rheumatoid arthritis and the comparative evaluation of the serum levels of the inflammatory cytokines (IL-4, IL-13) with lumbar T score in order to identify some useful correlations in the early diagnosis of some complications, and patients identification which can benefit from the specific treatment.
Patient’s selection
Since the diagnosis of psoriatic arthritis, due to the lack of universally accepted criteria, is quite difficult to determine, the number of patients with this diagnosis is relatively small, so our study was conducted on a relatively small number, but still representative for patients with diagnosis of psoriatic arthritis.
The number of patients in our study was influenced by the relatively limited opportunity to harvest synovial fluid from these patients. Thus, we included in the study only patients with psoriatic arthritis from which we could harvest both blood and synovial fluid from the affected joint.
The study was performed on three groups of patients:
Group 1 (patients with psoriatic arthritis diagnosed according to the criteria CASPAR (Classification Criteria for Psoriatic Arthritis) consists of 27 patients (n=27) including 15 men and 12 women, aged 27-50 years. Group 2 (patients with rheumatoid arthritis diagnosed according to the criteria of the American Rheumatology Association) consists of 21 patients (n=21) including 13 women and 8 men, aged 25-52 years. The control group (healthy subjects with a mean age of 30 years with rheumatic diseases, infectious, neoplastic or autoimmune) consists of 20 patients (n=20) including 9 women and 11 men.
Inclusion criteria
In our study we have included patients, aged 27-50 years, diagnosed with psoriatic arthritis based on CASPAR criteria (Classification Criteria for Psoriatic Arthritis) and rheumatoid arthritis diagnosed according to the criteria of the American Rheumatology Association. All patients had a mean duration of the disease of approximately 36 months, and were in acute phase of the disease and were not taking NSAIDs at least one month prior to inclusion in the study. For all these patients we performed a general clinical examination supplemented by laboratory investigations to exclude the presence of other autoimmune diseases related to a neoplastic process or a systemic infection.
Exclusion criteria
The patients with following conditions were excluded: ankylosing spondylitis, osteoarthritis, entezopatic seronegative arthropathy syndrome, enteropathic arthritis in colitis ulcerosa and Crohn’s disease, Behcet’s syndrome, Whipple disease, gout, lupus arthritis, septic arthritis, Leroy - Reiter syndrome Fiessinger, degenerative arthritis nodules, Heberden and Bouchard nodes, bone metabolism diseases diagnosed on the basis of a detailed case history, clinical examination and laboratory investigation (Paget’s disease, Cushing’s syndrome, multiple myeloma, lymphoma Hodgkin, etc); consumers of alcohol, malnutrition syndrome, vitamin D deficiency and treatment impact on bone metabolism, patients who received 12 months treatment with corticosteroids or methotrexate, other conditions that require treatment to long (over 6 months) glucocorticoid, patients who received the calcium supplement or vitamin D sustained physical activity in the past 12 months, women, age under 40 years, in early menopause of different etiology (surgical or medical).
From each patient we collected both peripheral blood and synovial fluid from the affected joint. The samples were stored at -70°C until measurements.
Determination of interleukin-4
The Interleukin 4 (IL-4) was determined by enzyme immunoassay with the sandwich ELISA technique (Enzyme Linked Immuno Assay sorbate), using ELISA kit Endogen, Woburg, MA, USA (sensitivity <2pg/ml, the accuracy of reproducibility between the determinations is CV<10%). The standard curve was constructed by means of six standards: 0 pg/ml, 10.24 pg/ml, 25.5 pg/ml, 64 pg/ml, 160 pg/ml and 400 pg/ml, were used for the determination of 50 mg of standards that samples (serum and synovial fluid), in duplicate. Reading was carried out with a “Human reader” at 450 nm without the use of differential filter, and the method of analysis used, was PGM.
Determination of interleukin-13
The Interleukin-13 (IL-13) was determined by enzyme immunoassay technique sandwich ELISA (Enzyme Linked Immuno Assay sorbate), using ELISA kit Medsystem Bender, Vienna, Austria (sensitivity <2 pg/ ml, precision reproducibility between measurements is CV=6.9%). The working technique followed the manufacturer’s instructions faithfully, on the one hand, and on the other hand, all determinations were made in parallel samples.
Determination of bone mineral density
The Bone mineral density was measured at the lumbar spine (L2- L4) using DEXA (dual-energy X-Ray absorptiometry) method. The osteopenia is defined on a T-score between -1 and -2 and T score ≤ -2.5 osteoporosis by WHO criteria and the NIH Consensus Conference, National Institutes of Health-2006.
Statistical analysis of the data
The statistics and the graphics in this study were made by using the Microsoft Office Excel 2007 using:
• the elements of descriptive statistics: arithmetic mean ± standard deviation (mean ± SD);
• the elements of inferential statistics: Student t test and Pearson test.
• Student t test was used to compare data from the two groups with the control group. We calculated the values of the coefficients: p1 (between group1 and control group), p2 (between group 2 and control group), p < 0.05 is statistically significant value.
• The Pearson test was used to compare data from the same batch analyzed. We calculated correlation coefficients: r1 (group 1), r2 (group 2), R3 (control group), r > 0.5- respectable correlation (positive or negative).
Serum levels of interleukin-4 (IL-4)
In both groups with psoriatic arthritis and rheumatoid arthritis the serum concentration of the interleukin- 4 for most patients showed no detectable values (20 cases). In other patients, these values were very low: 0.2 pg/ml 0.3 pg/ml 0.4 pg/ml 1.1 pg/ml 1.2 pg/ml, a maximum value of 1.4 pg/ml. This suggests that Th2 lymphocytes, in psoriatic arthritis and rheumatoid arthritis, are not active and do not secrete antiinflammatory cytokines that counteract the effects of proinflammatory cytokines secreted by Th1 lymphocytes. In the control group (healthy volunteers) the interleukin-4 was not detected in the serum, since the immunoinflammatory activity which require the activation of the Th2 lymphocytes, that secrete anti-inflammatory, and the cytokines to counter the action of proinflammatory cytokines do not exist.
The level of interleukin 4 measured in synovial fluid from patients with psoriatic and rheumatoid arthritis
In group 1 the level of interleukin-4 had a value between 0.20 and 0.50 pg/ml (mean of 0.41 ± 0.08 pg/ml).
In group 2 the level of interleukin-4 had a value between 0.58 and 0.70 pg/ml (mean of 0.63 ± 0.09 pg/ml) (Figure 1).
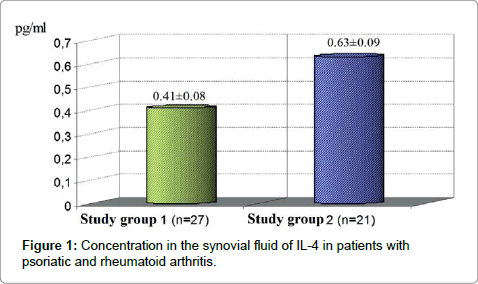
Figure 1: Concentration in the synovial fluid of IL-4 in patients with psoriatic and rheumatoid arthritis.
As can be seen, in the synovial fluid concentration of interleukin-4 is higher in psoriatic arthritis compared to rheumatoid arthritis, which corresponds to the results of the studies cited in the literature, meaning that, at this level, the higher concentration of pro-inflammatory cytokines is in rheumatoid arthritis, and thus more significant increase of these anti-inflammatory cytokines try to counteract the effects exerted by proinflammatory cytokines.
Comparison of the levels of interleukin 13 in serum and synovial fluid from patients with psoriatic and rheumatoid arthritis
In group 1 the concentration of IL-13 had the following values: serum between 2.67 and 4.99 pg/ml (mean 1.45 ± 3.22 pg/ml), p1 < 0.01-S, statistically significant compared with control group) and in the synovial fluid values between 2.07 and 14.8 pg/ml (mean 5.8 ± 0.45 pg/ ml).
In group 2 the concentration of IL-13 had the following values: serum between 2.21 and 13.32 pg/ml (mean 10.2 ± 1.48 pg/ml p2 < 0.002, ES, highly statistically significant compared with control group) and in the synovial fluid values between 2.11 and 18.8 pg/ml (mean 6.7 ± 1.08 pg/ml) (Figure 2).
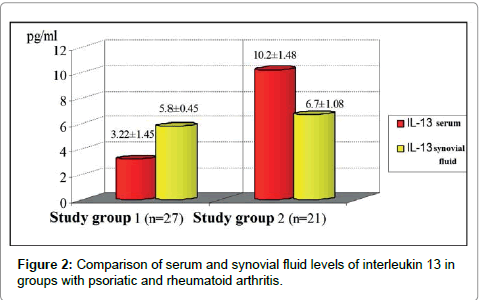
Figure 2: Comparison of serum and synovial fluid levels of interleukin 13 in groups with psoriatic and rheumatoid arthritis.
These personal results, studied and cited in the literature come to show that IL-13 level in psoriatic arthritis synovial fluid is higher than in the blood, so there is a local secretion of this cytokine in the affected joint.
It can be said therefore that IL-13 secretion profile is different for distinct types of arthritis.
The anti-inflammatory cytokine levels in synovial fluid compared in patients with psoriatic and rheumatoid arthritis
In group 1 the level of IL- 4 had a value between 0.20 and 0.50 pg/ ml (mean of 0.41 ± 0.08 pg/ml) and IL-13 had the values between 2.07 and 14.8 pg/ml (mean 5.8 ± 0.45 pg/ml).
In group 2 the level of IL-4 had a value between 0.58 and 0.70 pg/ml (mean of 0.63 ± 0.09 pg/ml) and IL-13 had the values between 2.11 and 18.8 pg/ml (mean 6.7 ± 1.08 pg/ml) (Figure 3) .
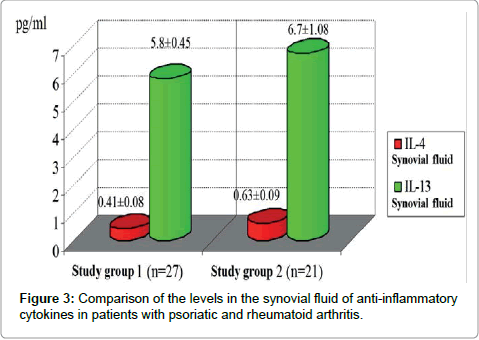
Figure 3: Comparison of the levels in the synovial fluid of anti-inflammatory cytokines in patients with psoriatic and rheumatoid arthritis.
Comparative evaluation of serum levels of anti-inflammatory cytokines with bone mineral density values
In group 1 serum IL-4 in most patients showed no detectable serum concentration, and IL- 13 had values between 2.67 and 4.99 pg/ml (mean 1.45 ± 3.22 pg/ml) p1 < 0.01-ES, statistically significant compared to control group), and the lumbar T score was ranged between 1.58 and 1.77 DS (mean -1.68 ± 0.06 SD; P’1 < 0.01- ES, statistically significant compared to control group).
In group 2 serum IL-4 in most patients showed no detectable serum concentration, and IL-13 had values between 2.21 and 13.32 pg/ml (mean 10.2 ± 1.48 pg/ml p2 < 0.002 -ES highly statistically significant compared to control group), and the lumbar T score had values between -2.51 and -3.41 DS (average of -2.93 ± 0.3 SD, p’2 < 0001-ES, highly statistically significant compared to control group).
In the control group IL-4 was not detected in serum, and serum IL-13 had values between 2.05 and 3.35 pg/ml (mean 0.51 ± 2.12 pg/ ml), and the lumbar T score had value between 0.29 and 1.3 DS (mean 0.82 ± 0.32 SD) (Table 1, Figures 4-6).
| Parameters (mean±SD) | Study group 1 (n=27) | Control group (n=20) | Study group 2 (n=21) |
| Lumbar T score (SD) | -1.68±0.06 p1’<0.01 | 0.82±0.32 | -2.93±0.3 p2< 0.001 |
| IL-13 serum (pg/ml) | 3.22±1.45 p1<0.01 r1=0.68 | 2.12±0.51 r3=0.71 | 10.2±1.48 p2<0.002 r2=0.82 |
Table 1: Comparison of serum levels of IL-13 and T- lumbar score for the groups analysed.
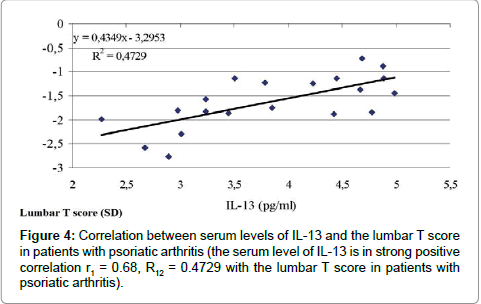
Figure 4: Correlation between serum levels of IL-13 and the lumbar T score in patients with psoriatic arthritis (the serum level of IL-13 is in strong positive correlation r1 = 0.68, R12 = 0.4729 with the lumbar T score in patients with psoriatic arthritis).
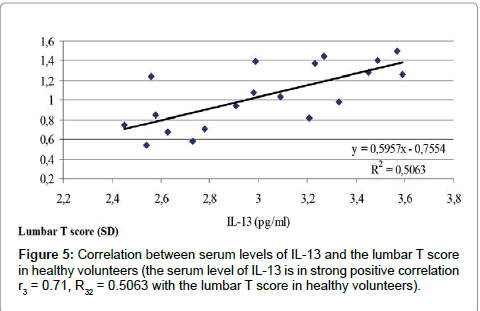
Figure 5: Correlation between serum levels of IL-13 and the lumbar T score in healthy volunteers (the serum level of IL-13 is in strong positive correlation r3 = 0.71, R32 = 0.5063 with the lumbar T score in healthy volunteers).
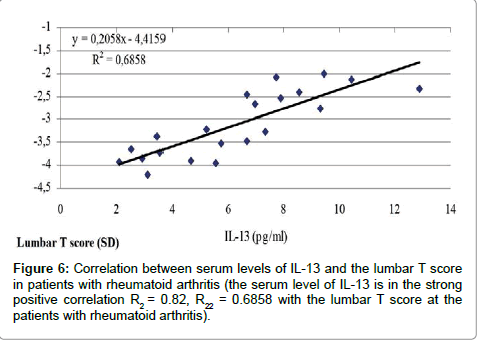
Figure 6: Correlation between serum levels of IL-13 and the lumbar T score in patients with rheumatoid arthritis (the serum level of IL-13 is in the strong positive correlation R2 = 0.82, R22 = 0.6858 with the lumbar T score at the patients with rheumatoid arthritis).
Table 1 show that there is a strong positive correlation between blood values of IL-13 and lumbar T score values both in patients with psoriatic arthritis and in those with rheumatoid arthritis.
The cytokines secreted by T cells play a major role in the induction and maintenance of synovial inflammation. The anti-inflammatory cytokines secreted by activated T lymphocytes, and in particular IL-13 is the modulator factor of inflammation in the autoimmune diseases [14].
The results of the comparative study regarding the role of the interleukin-13 in psoriatic arthritis and rheumatoid arthritis showed that this cytokine causes besides anti-inflammatory and growth inhibitory action of synoviocytes, collagenase reduction and augmentation IL-1 Ra synthesis by synoviocytes [13].
Also, these studies have shown that the blood levels of the cytokine are significantly higher than in healthy control group in psoriatic arthritis compared to rheumatoid arthritis, where the concentration of interleukin- 13 is much higher, and the blood levels of interleukin-13 in patients with rheumatoid arthritis correlate well with the levels in the synovial fluid, becoming higher, correlation which does not exist in psoriatic arthritis, where blood levels of interleukin-13 are not greatly increased [11].
In order to assess the role of Th2 lymphocytes in psoriatic arthritis in our study we determined the concentration at the joint fluid and serum of the interleukin-4, the prototype of Th2 cytokines, and interleukin- 13, and compared the results with those obtained from healthy serum and from synovial fluid of patients with rheumatoid arthritis.
In our study we included patients with psoriatic arthritis whom were in the acute phase of the disease because we assumed that at this stage cytokine profile changes are most pronounced, being evident not only in the affected joints but also in the patient’s serum.
Our results demonstrate that in peripheral blood from healthy control group interleukin-4 is not highlighted. It is considered that our results fall within the normal serum levels of this cytokine, because the results of the ELISA kits (Endogen Inc.) also indicate undetectable serum levels in healthy individuals investigated, considering them normal.
In groups with psoriatic arthritis and rheumatoid arthritis the serum levels of interleukin-4 are extremely low, sometimes below detection value of the kits we used. These results demonstrates that Th2 lymphocytes are activated and they secrete anti-inflammatory cytokines that counterbalance the effects of proinflammatory cytokines secreted by Th1 lymphocytes.
Our research revealed also that the blood levels of interleukin-13 are increased in patients with both rheumatoid arthritis and in patients with psoriatic arthritis, but the difference compared to the control group is not very high (but still statistically significant).
Corroborating our findings on the profile of serum antiinflammatory cytokines can be said that Th2 cell activation in psoriatic arthritis and the anti-inflammatory cytokine secretion, used to keep the balance Th1/Th2, is not optimal.
In the synovial fluid the interleukin-4 and interleukin-13 were found in both groups of the patients studied (psoriatic arthritis and rheumatoid arthritis). The differences were the significantly lower values of the interleukin 4 and interleukin 13 in patients with psoriatic arthritis than those with rheumatoid arthritis. We also found that in patients with psoriatic arthritis there is an increase in the ratio of the concentration of IL-13 in synovial fluid and blood as opposed to those with rheumatoid arthritis. These data lead to the logical conclusion that in psoriatic arthritis exist a local production of interleukin-13 in the inflamed joint.
These results are not surprising, the personal interest in studying the anti-inflammatory cytokines starts from the known fact that IL- 13 production depends on activated helper T cells, lymphocytes that play an important role both in the psoriatic arthritis and rheumatoid arthritis. In both types of arthritis, the number of T helper lymphocyte is increased in blood as in the synovial fluid, but there are some differences. Thus, in patients with rheumatoid arthritis, at blood level, there is an excess of helper T cell type CD4 and a deficit of T-lymphocytes type CD8, facts that are not seen in psoriatic arthritis and in healthy control group [13].
The CD4 T lymphocytes are the predominant subset in the synovial tissue of arthritis, but, paradoxically, do not exist in the synovial fluid. This can be explained by the difference between the number and the activation status of these cells or by the evolution phases of the disease [11,13].
All these results of the studies cited in the literature confirm that the differences existing at the joint levels between the rheumatoid and psoriatic arthritis are more quantitative than qualitative.
This is demonstrated by our results which showed that in the synovial fluid, the cytokine pattern secreted by activated T lymphocytes is similar in the rheumatoid and psoriatic arthritis, the differences being their lower concentration in psoriatic arthritis.
Our study has shown that there are significant differences regarding the profile of anti-inflammatory cytokines from serum and synovial fluid of patients with psoriatic arthritis versus healthy controls and patients with rheumatoid arthritis.
While in the blood of healthy patients the presence of interleukin was not detected, in patients with psoriatic arthritis and rheumatoid arthritis its concentration was very low, in some cases below the detection limit of the kit used. It can be concluded therefore, that in the blood of the patients with psoriatic arthritis and rheumatoid arthritis exists a lack of anti-inflammatory cytokines, which makes it impossible to maintain Th1/Th2 balance.
In the synovial fluid, however, for both types of arthritis was identified the presence of interleukin-4 in a concentration higher than that psoriatic rheumatoid arthritis, which is not reflected by blood levels of the interleukins. These results lead to the logical conclusion that there is a local synthesis of interleukin-4.
Thus, our study shows that the pattern of local or systemic production of IL-13 may influence the clinical picture of the arthritis with the occurrence of psoriatic arthritis, and rheumatoid arthritis, respectively reflecting the existence of different pathogenic mechanisms involved in inflammatory joint diseases.
Our study personal contribution consists in demonstrating that in the blood of psoriatic arthritis patients there is not a necessary and sufficient production of anti-inflammatory cytokines (IL-4 is below the detection limit of the kit used and IL-13 shows similar results to those of healthy patients used as witnesses), so that Th1/Th2 levels cannot be balanced. It follows therefore that for psoriatic arthritis counter in blood level of proinflammatory cytokine is not optimal. Analysing these results it can be stated that interleukin 13 may find a role in the therapeutic arsenal of the psoriatic arthritis as has been demonstrated in different animal models.
Our study by determining blood interleukin-13 showed no significant changes between patients with psoriatic arthritis (mean 3.22 ± 1.45 pg/ml, p1<0.01) and healthy control groups (2.12 ± 0.51 pg/ml), while in patients with rheumatoid arthritis this cytokine concentration is much higher (10.2 ± 1.48, p2<0.002) as compared to healthy control group and patients with psoriatic arthritis.
In synovial fluid our results showed an increased concentration of IL-13 in rheumatoid arthritis against psoriatic arthritis. While in rheumatoid arthritis the synovial fluid levels of IL-13 in the peripheral blood is correlated, this is not the case in patients with psoriatic arthritis, those patients having an increased ratio of IL-13 synovial fluid/blood, which shows local production of this cytokine.
