Research Article - (2016) Volume 5, Issue 5
Osteoarthritis (OA) is the common form of chronic musculoskeletal degenerative joint disease in elder population and earlier studies have correlated the OA with genetics. The aim of this current study was analyse the collagen linked variants such as COL2A1 (rs73297147), CRTL1 (rs73771337), and CRTM (rs74063376) gene polymorphism with clinically diagnosed and radiologically confirmed primary knee osteoarthritis in south Indian population. Two hundred genomic DNA samples were isolated from 100 primary knee OA cases and 100 healthy controls. Genomic DNA was isolated from peripheral blood sample and followed by PCR-RFLP analysis. A significant difference was observed in allele and dominant model in COL2A1 gene polymorphism (G vs A: p=0.01 (OR-1.10-2.48) OR=6.01) and (GG+AG: p=0.001 (OR-1.41-4.74) OR=2.6) within cases and controls. The T allele and TT+GT genotype of CRTL1 gene polymorphism was seen to be a significant difference (G: p=0.005 (OR-1.27-4.64) OR=2.43) and (TT+GT: p=0.01 (OR-1.2-4.74) OR=2.38). The CRTM polymorphism was negatively associated with all alleles and genotypes (p>0.05). GMDR interaction model supports the correlation among these 3 variants. The current results indicate that the rs73297147, rs73771337 polymorphisms in COL2A1 and CRTL1 genes could be associated with developing primary knee OA in south Indian population.
Keywords: Knee osteoarthritis; COL2A1; CRTL1; CRTM; Gene polymorphism
The osteoarthritis (OA) or degenerative joint disease is a progressive musculoskeletal disorder prone in elderly population. The disease OA itself is an active inflammatory condition and promises to remain a significant cause for pain and disability [1]. Age, genetics and environmental factors are the main risk factors for the cause of primary OA [2] and genetics is estimated to cause 30% risk for the development of the disease [3]. Knee OA is a mechanically driven disease with degenerative arthritis, proposed to be medial tibiofemoral kneejoint load increases with pharmacologic pain relief. The underlying mechanisms are still unknown and genetic factors contribute the development of OA the heritability has been estimated at 48%–65% [4].
The evidence of epidemiological studies proposes aging, genetic predisposition, obesity, inflammation and excessive mechanical loading predispose to OA development. Furthermore, the identification of candidate genes and pathways would help elucidate the molecular mechanisms of OA to have the potential to evaluate the risk for OA and lead to the development of OA gene-targeted therapies [5]. The genetic indication in OA cases originates from twin, family and animal model studies. Currently, the majority of genetic association studies on osteoarthritis disease risk focused on identifying the individuals effect on single nucleotide polymorphisms (SNPs) as well as their interaction effects on the disease. Based on genome-wide association studies (GWAS), twenty-one OA susceptibility loci have been established individually (P ≤ 5×10-8) and with established functional association in OA from continuation studies [6,7]. Although some SNPs in numerous genes have been projected as OA susceptibility loci and few of them established in replication studies due to the genetic heterogeneity of OA. The documentation of candidate genes has essentially focused on encoding genes collagen, particularly type II collagen, and other structural proteins of cartilage extracellular matrix; bone and cartilage growth factors. Few genes deceive the occurrence and development of OA mainly regulate the formation, degradation and repair of articular cartilage or subchondral bone metabolism [8-13]. Genes predominantly encoding structural proteins of the extracellular matrix include collagen type II alpha 1 (COL2A1), cartilage link protein (CRTL1), and cartilage matrix protein (CRTM) genes that have been evaluated in the present study [11,14]. The aim of the current study was to analyze the collagen variants such as COL2A1 (A28602G; rs73297147), CRTL1 (G8206T; rs73771337), CRTM (A1412C; rs74063376) with clinically diagnosed knee osteoarthritis cases in south Indian population.
Altogether, 200 South Indian individuals were recruited from Kamineni Hospitals, Hyderabad and India. The 100 primary knee OA cases were treated in the Department of Orthopedics and 100 healthy controls were recruited from master health checkup clinic. Adult OA cases were enrolled with the confirmation of clinical diagnosis and radiological score with 1-4 in Kellgren and Lawrence scale [15]. This case-control study was initiated with the institutional ethical approval and clinical, medical and family histories were documented in a welldesigned proforma. The inclusion and exclusion criteria of both the cases/controls were informed in our prior studies [4,16]. We acquired 2 ml of the peripheral blood in an EDTA vacationer for extraction of genomic DNA from salting out technique, routinely used in our NABL accreditation laboratory [17]. Randomly 50 ul of Tris-EDTA buffer was used to solidify the genomic DNA and NanoDrop was used to measure the DNA quality (NanoDrop 2000, Thermo Fisher Scientific, MA, USA) [18]. Molecular analysis was performed by designing the specific primers for COL2A1 (A28602G), CRTL1 (G8206T), and CRTM (A1412C) candidate genes. Genotyping was done with the PCR and RFLP analysis. The protocol of the PCR has been described in our prior publications [19]. The PCR products were digested with precise restriction enzymes describes in Table 1 and followed by agarose gel electrophoresis.
| Gene | SNP | rs no | Band | Forward primer | Reverse primer | PCR Amplicon | Fragment Sizes (bp) |
|---|---|---|---|---|---|---|---|
| COL2A1 | A28602G | rs73297147 | 12q13 | TGAAGGAGAAGGTGTCTGCGGGA | GGACGGTGCGGTGAGAGTG | 167 bp | A-167bp G-143/24 bp |
| CRTL1 | G8026T | rs73771337 | 5q14 | TCAGGCAGGAACAACACCAT | GGTTACTTCAAGGACAAAATACCTGTAAAGCT | 249 bp | G-249 bp T-159/90 bp |
| CRTM | A1412C | rs74063383 | 1p35 | CTGGAGACCACTCCCATCCTTTCT | GATGTGGCCATCACATTCGTCACGAT | 237 bp | A-237 bp C-143/94 bp |
Table 1: Candidate gene SNPs and primers used in this study.
Baseline clinical data are documented as mean ± standard deviation (M ± SD). The allele and genotypic associations between OA cases and controls were observed with odds ratio (OR) and 95% confidence interval followed by chi-square analysis. The middleaged anthropometric, baseline and clinical characteristics has been documented in Table 1. Openepi software was used to accomplish the power calculation [20]. The genotypes for Hardy–Weinberg equilibrium (HWE) was intended by consuming OEGE (online encyclopedia calculator for genetic epidemiology studies) [21]. A p value of <0.05 was considered significant. Multifactor dimensionality reduction (MDR) and Generalized Multifactor dimensionality reduction (GMDR) model was implemented with prior study by Khan et al. [22].
The present clinical data confirmed the negative association with gender (sex) and age (p=0.88 and p=0.87). The anthropometric information is organized in Table 2. The other body factors such as weight (0.001) and BMI (0.01) were associated in the predisposition of disease with the cases and controls. Furthermore, 28% of the cases had the family history of OA and 50% were undergoing treatment for hypertension. Genotypic and allelic distributions of all the polymorphisms satisfied HWE. Table 3 represents the proportion of allele and genotype frequencies in all the 3 polymorphisms in OA cases and controls. The allele data for COL2A1 (A28602G) and CRTL1 (G8206T) polymorphisms yielded positive association (P=0.01; OR=1.65, 95%CI 1.10–2.48; P=0.005; OR=2.43, 95%CI 1.27–4.64) and CRTM (A1412C) turns to be negative association (P=0.20; OR=2.38, 95%CI 0.60–9.34). Assessed polymorphisms for COL2A1 (A28602G) and CRTL (G8206T) was associated with either genotype frequencies and or with dominant model between the cases and controls. The heterozygous genotypes in A28602G and G8206T polymorphisms were associated significantly (OR-2.66, P=0.02; 95%CI (1.41-4.99) and OR-2.27; 95% CI: 1.14-4.51), P=0.02). We observed the parallel similarity with the dominant model of genotype i.e. (GG+AG: p=0.001 (OR-1.41-4.74) OR=2.6; TT+GT: p=0.01 (OR-1.2-4.74) OR=2.38). For the polymorphism CRTM (A1412C), there was no evidence of the association either in allele form or genotype frequencies with the risk of OA, which was observed for rs74063376 polymorphism after yates’ correction (P=0.2153; OR=2.235, 95%CI:0.609-8.199 and P=0.98; OR=1.04, 95%CI:0.02-53.1).
| Characters | Cases (n=100) | Controls (n=100) | p Value |
|---|---|---|---|
| Age (Years) | 42.41 ± 8.11 | 42.17 ± 7.98 | 0.87 |
| Sex: (M:F) | 29:71 | 31:69 | 0.88 |
| Height (cms) | 156.63 ± 2.68 | 155.46 ± 2.45 | 0.37 |
| Weight (kg) | 76.97 ± 8.44 | 69.78 ± 7.87 | 0.001 |
| BMI (kg/m2) | 31.38 ± 3.4 | 25.89 ± 2.67 | 0.01 |
| Age of Onset | 39.52 ± 6.89 | NA | NA |
| History of HTN | 50 (50%) | 15 (15%) | <0.01 |
| History of T2DM | 38 (38%) | 14 (14%) | <0.01 |
| History of Thyroid dysfunction | 39 (39%) | 22 (22%) | <0.01 |
| NA=Not applicable | |||
Table 2: Clinical characteristics of OA cases and controls.
| Genotypes | OA Cases | Controls | Odds ratio (95% CI) | χ2 | p value |
|---|---|---|---|---|---|
| COL2A1(A28602G) | |||||
| AA | 24 (24%) | 45 (45%) | |||
| AG | 61 (61%) | 43 (43%) | 2.66 (1.41-4.99) | 9.4 | 0.002 |
| GG | 15 (15%) | 12 (12%) | 2.34 (0.94 -5.80) | 3.43 | 0.06 |
| A | 109 (0.545) | 133 (0.665) | |||
| G | 91 (0.455) | 67 (0.335) | 1.65 (1.10-2.48) | 6.01 | 0.01 |
| CRTL1 (G8026T) | |||||
| GG | 70 (70%) | 85 (85%) | |||
| GT | 27 (27%) | 15 (15%) | 2.27 (1.14-4.51) | 4.81 | 0.02 |
| TT | 03 (03%) | 00 (0%) | 8.48 (0.43-167.1) | 2.79 | 0.09* |
| G | 167 (0.835) | 185 (0.925) | |||
| T | 33 (0.165) | 15 (0.075) | 2.43 (1.27-4.64) | 7.65 | 0.005 |
| CRTM (A1412C) | |||||
| AA | 93 (93%) | 97 (97%) | |||
| AC | 07 (07%) | 03 (03%) | 2.43 (0.61-9.7) | 1.67 | 0.19 |
| CC | 00 (00%) | 00 (00%) | 1.04 (0.02-53.1) | 0.0004 | 0.98* |
| A | 193 (0.965) | 197 (0.985) | |||
| C | 07 (0.035) | 03 (0.015) | 2.38 (0.60-9.34) | 1.63 | 0.2 |
| *Yates correction | |||||
Table 3: Genotype and allele frequencies for the evaluated genes.
The genotype and allele frequencies of COL2A1 (A28602G), CRTL1 (G8206T), and CRTM (A1412C) polymorphisms was not associated within the gender stratification. However, Table 4 describes the statistical calculation for allele and genotype frequencies amongst the males and females of the OA patients.
| Genotypes | Females (n=71) | Males (n=29) | Odds ratio (95% CI) | p value |
|---|---|---|---|---|
| COL2A1 (A28602) | ||||
| AA | 08 (11.3%) | 16 (55.2%) | ||
| AG | 52 (73.2%) | 09 (31%) | 0.08 (0.02-0.26) | 0.002 |
| GG | 11 (15.5%) | 04 (13.8%) | 0.18 ( 0.04-0.75) | 0.01 |
| A | 68 (0.48 ) | 41 (0.70) | ||
| G | 74 (0.52) | 17 (0.30) | 0.38 (0.2-0.7) | 0.003 |
| CRTL1 (G8026T) | ||||
| GG | 47 (66.2%) | 23 (79.3%) | ||
| GT | 22 (31%) | 05(17.2%) | 0.46 (0.15-1.38) | 0.16 |
| TT | 02 (2.8%) | 01 (3.5%) | 1.0 (0.08-11.86) | 0.98 |
| G | 116 (0.82) | 51 (0.88) | ||
| T | 26(0.18) | 7 (0.12) | 0.61 (0.24-1.50) | 0.28 |
| CRTM (A1412C) | ||||
| AA | 66 (93%) | 27 (93.1%) | ||
| AC | 05 (7%) | 02 (6 9%) | 0.97 (0.17-5.35) | 0.97 |
| CC | 00 (0%) | 00 (0%) | 2.41 (0.04-124.9) | 0.65 |
| A | 137 0.97) | 56 (0.965) | ||
| C | 05 (0.03) | 02 (0.035) | 0.97 (0.18-5.2) | 0.97 |
*Yates correction
Table 4: Genotype and allele frequencies of OA males and OA females.
One-three-way interaction of gene-gene model was listed in Table 5. In this study, general multi dimensionality reduction (GMDR) software was applied to discover the gene-gene interactions within the 3 SNPs. The current GMDR results confirms the single (rs73297147; P=0.05, Cross validation consistency was 10/10; testing balancing accuracy was 60.3%) and three-locus (rs73297147 rs73771337 rs74063376; P=0.05, Cross validation consistency was 10/10; testing balancing accuracy was 58.5%) model as the positive association in the OA disease. However, we could find the significant association with two-locus (rs73297147 rs73771337; P=0.17, Cross validation consistency was 05/10; testing balancing accuracy was 57.5%) of GMDR model.
| BMI | OA Cases (n=100) | BMI (Mean ± SD) | Genotypes-COL2A1 | ||
|---|---|---|---|---|---|
| AA | AG | GG | |||
| Normal (0-24.9) | 6 | 23.42 ± 1.19 | 1(16.7%) | 4(66.6%) | 1 (16.7%) |
| Overweight (25.0-29.9) | 24 | 28.56 ± 0.94 | 5(20.8%) | 12 (50%) | 7 (29.2%) |
| Obese (>30.0) | 70 | 33.18 ± 3.40 | 10(14.3%) | 52(74.3%) | 8 (11.4%) |
| OA Cases (n=100) | BMI (Mean±SD) | Genotypes-CRTL1 | |||
| GG | GT | TT | |||
| Normal (0-24.9) | 6 | 23.42 ± 1.19 | 5(83.3%) | 1(16.7%) | 0 (0%) |
| Overweight (25.0-29.9) | 24 | 28.56 ± 0.94 | 19(79.2%) | 4 (16.7%) | 1(4.1%) |
| Obese (>30.0) | 70 | 33.18 ± 3.40 | 43(61.4%) | 25(35.7%) | 2 (2.9%) |
| OA Cases (n=100) | BMI (Mean±SD) | Genotypes-CRTM | |||
| AA | AC | CC | |||
| Normal (0-24.9) | 6 | 23.42 ± 1.19 | 6(100%) | (0%) | 0 (0%) |
| Overweight (25.0-29.9) | 24 | 28.56 ± 0.94 | 22(91.7%) | 2 (8.3%) | 0 (0%) |
| Obese (>30.0) | 70 | 33.18 ± 3.40 | 66(94.3%) | 4(5.7%) | 0 (0%) |
Table 5: Association between BMI and genotypes of specific cartilage genes component-encoding genes evaluated in this study.
An entropy graph obtained after MDR analysis showed interactions of gene polymorphisms with other anthropometric parameters and clinical features in primary knee OA compared to controls. BMI (14.09%), type 2 diabetes (5.11%), hypertension (9.89%), and thyroid dysfunction (2.24%) contributed to primary knee OA. BMI contributed most to disease pathology and has strong synergistic interaction with the COL2A1 G allele with an entropy of 2.83%, redundancy with hypertension and thyroid dysfunction (Figure 1).
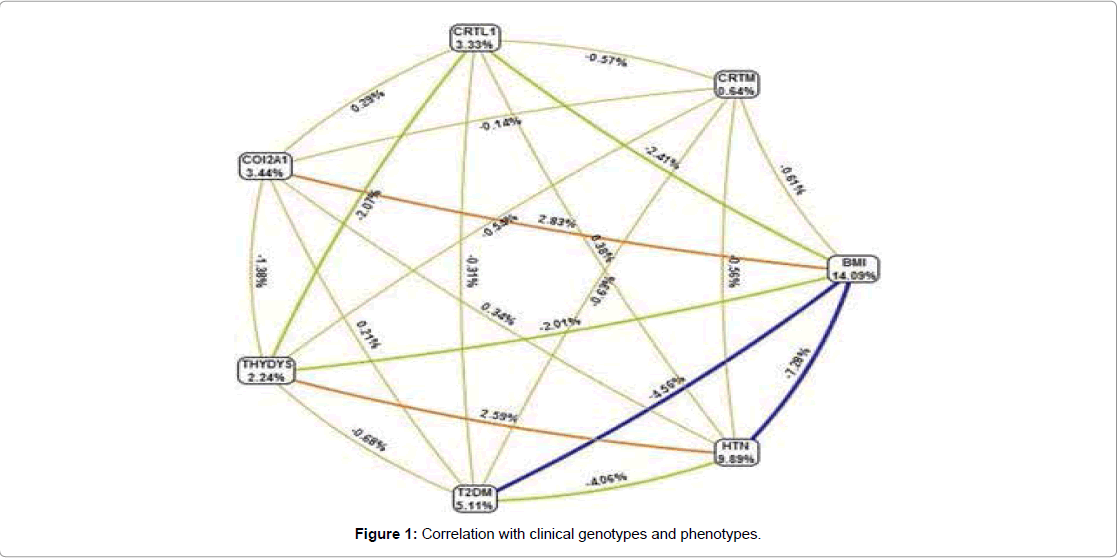
Figure 1: Correlation with clinical genotypes and phenotypes.
Genetic association of COL2A1 (A28602G), CRTL1 (G8206T) and CRTM (A1412C) polymorphic variants with primary knee OA risk and aggressiveness were investigated in this hospital based casecontrol study in South Indian population. The variants for A28602G and G8206T were associated with AG and GT genotypes appeared 2.3 and 2.2 fold increased risk for primary knee OA. However, we could not identify the significant difference with A1412C genotype frequency within the cases and controls. Also, there was no gender difference between the OA cases and controls in three gene polymorphisms.
OA has converted as joint disorder and a leading cause of disability in elderly population and the early onset of OA has prone to be major risk issue in knee OA [23,24]. The involvement between genetics and OA has been broadly scrutinized in linkage, association and family based studies. Genetic association studies have helped in recognizing the effects of precise gene variants on OA pathogenesis, but had only minor effects specifying the complex polygenic nature of OA [25]. The exposure of OA is coded with DNA polymorphism and as such these studies involved a comparison of the frequency of polymorphisms in individuals with the disease versus those with disease-free controls, or those in whom osteoarthritis status had not been determined. Such case-control studies have tremendous power, so long as certain criteria are encountered [26].
The selection of COL2A1 candidate gene is due to the effect of protein in the articular cartilage. Mutations in COL2A1 affect joint function, bone development and cause hereditary cartilage diseases and type II collagen encodes the COL2A1 protein, most abundant in articular cartilage and intervertebral disk, an additional vital protein elaborated with expansion of OA [27]. Meulenbelt et al. [28] was the initial study conceded the positive association with COL2A1 gene with hip and knee OA in Rotterdam study. Earlier studies on COL2A1 association with OA and knee OA were conducted in populations of different ethnicities [11,27-31].
The cartilage link proteins such as CRTL1 and CRTM stabilizes proteoglycan aggregates through binding both the proteoglycan core protein and to hyaluronic acid [11]. The CRTL1 protein appears in the non-collagenous extracellular matrix also contributes the etiology of OA disease. The gene CRTL1 stabilizes proteoglycan aggregates by binding to both the proteoglycan core protein and hyaluronic acid [32,33]. CRTM encodes a major protein component appear in the non-articular cartilage of the extracellular matrix fixes to collagen. The mutation G8206T (rs7772941) in CRTM have been associated with variety of inherited chondrodysplasias. CRTM polymorphisms were not associated with primary knee OA (A1412C: OR=2.43, 95% CI=0.61–9.7, p=0.19 and OR=2.38, 95% CI=0.60–9.043, p=0.20). Meulenbelt et al. [11] conducted a study on associations in Rotterdam population between CRTM and CRTL1 and generalized OA, and concluded as CRTM locus may play a role in OA in a gender- and joint site-specific manner. Our results were not in agreement with those of Meulenbelt et al. [11,28], as our results showed an association of OA with CRTL1 but not with CRTM. This may be due to differences in ethnicity of studied populations and the BMI, a well-established risk factor for weight gain in patients with OA.
We have categorized OA cases based on BMI into (i) 18.5–24.9 BMI as normal, (ii) 25.0–29.9 BMI as overweight and (iii) >30 BMI as obese groups as BMI is one of the major factor contributing for the disease pathology. The mean BMI for normal and overweight groups were 23.42 ± 1.19 and 28.56 ± 0.94, respectively. The mean BMI for the obese group was 33.18 ± 3.40 (Table 5). The prevalence of obesity in the AG genotype of the COL2A1 (A28602G) polymorphism was 74.3%, whereas that in GG and AA genotypes of CRTL1 (G8206T) and CRTM (A1412C) polymorphisms was 61.4% and 94.3%, respectively. Homozygous (AA), heterozygous, and obese variant genotypes of COL2A1 contribute significantly to the heritability of primary knee OA. From our analysis, we detected around 70% of abnormal BMI patients detected with G and T alleles in COL2A1 and CRTL1, respectively. However, the OA patients with <25 kg/m2 BMI possessed deleterious alleles. The ANOVA analysis revealed the significant association between BMI and genotypes (p<0.05). The prior study from our group within the OA patients exhibited the positive association with ACE I28005D polymorphism [16]. This study accomplishes that obese patients are at a higher risk for OA in south Indian population.
Gene-Gene and Gene-environment connections were analyzed with MDR statistical tool, a method used for combining high dimensional genetic data into a single dimension, which permits interactions to be detected in relatively small samples [22]. MDR analysis was conducted to find interactions among genotypes of OA cases and controls with demographic parameters. The results of MDR indicated that COL2A1 (rs73297147) and combination of three SNPs i.e., (rs73297147+rs73 771337+rs74063376) contribute to pathogenesis of OA and discloses strong interaction.
The limitations of our present study comprises that we have analyzed only one SNP from each gene. In conclusion, our study showed that A28602G and G8206T polymorphisms in COL2A1 and CRTL1 genes were significantly associated with primary knee OA in the South Indian population.
The authors extend their appreciation to the Kamineni Hospitals for funding this research.
There is no conflict of Interest towards this article.
