Research Article - (2014) Volume 3, Issue 1
Aim: The aim of the present study was to investigate the impact of Neutrophil-Lymphocyte Ratio (NLR) on Coronary Flow Reserve (CFR) and incipient myocardial dysfunction in patients with Psoriatic Arthritis (PsA) without risk for coronary artery disease.
Methods and results: We analyzed clinical, hematologic, echocardiographic and CFR data of 68 patients (mean age 41.5 ± 8.2years), who had no risk factor for coronary artery disease. Sixty-two healthy subjects were served as control group. NLR was significantly higher in patients with PsA versus control subjects (7.86 ± 0.6 vs. 1.39 ± 0.6, P<0 .0001). CFR was significantly lower in patients with PsA than in control subjects (1.9 ± 0.3 vs. 3.6 ± 0.2; P <0.002). The myocardial function was significantly impaired in patients than control subjects (E/E’ was 12.3 + 0.7 vs. 5.3 ± 0.8; P<0.01 and Sm was 3.9 ± 0.3 vs. 8.9 ± 0.5; P<0.01). NLR was significantly negatively correlated with CFR (r=- 0.73, P<0.0001); Sm (r=0.43; P<0.03), and positively correlated with E/E’ (r=0.57; P<0.001). Using multiple logistic regression analysis, NLR, and C-reactive protein levels emerged as independent predictors of impaired CFR, elevated E/E’ and decreased Sm. In receiver operating characteristics curve analysis, NLR ≥ 3.2 and ≥ 3.6 were the cut-offs in predicting impaired CFR and increased E/E’ in patients with PsA.
Conclusion: High NLR is a powerful and independent predictor of impaired CFR and incipient myocardial dysfunction in patients with psoriasis arthritis.
Keywords: Neutrophil-lymphocyte ratio, Coronary flow, Myocardial function, Psoriasis
Psoriasis is a hereditary, chronic inflammatory skin disorder and Psoriatic Arthritis (PsA), which has been defined as an inflammatory arthritis associated with psoriasis, appears to be linked to increased cardiovascular mortality and morbidity [1]. Several factors might explain the raised cardiovascular risk: smoking, hypertension, reduced physical activity, an altered lipid profile, chronic inflammation with elevated levels of inflammatory factors (e.g., platelet-activating factor), hyperhomocysteinemia or hypercoagulability [2-4].
Inflammation and the accompanying elevation in the homocysteine and C -reactive protein (CRP) levels, the increased platelet activation, and cytokine imbalance between coagulation-fibrinolysis seem to be responsible for this relationship. The increase in the incidence of classic atherosclerotic risk factors and treatment with immunosuppressive agents contribute to the development of atherosclerosis in patients with psoriasis [5,6]. Proinflammatory cytokines produced by type 1 T-helper lymphocytes such as TNF-α and interferon are important participants in plaque formation and in the development of endothelial dysfunction and atherosclerosis in patients with psoriaticarthritis [7,8].
A better knowledge of the association between PsA and cardiovascular comorbidities can help in early management and modification of risk factors, minimize the impact of the cardiovascular comorbidities, and improve patients’ long-term outcome. So we aimed to evaluate the impact of neutrophil-lymphocyte ratio on coronary flow reserve and incipient myocardial dysfunction in patients with psoriatic arthritis.
For the purposes of this study, 68 consecutive patients with psoriatic arthritis (49 males, 19 females; mean age 41.5 ± 8.2 years) and 62 healthy, sex- and age- matched individuals (45 males, 17 females; mean age 42.6 ± 7.6 years) were enrolled between October 2010 and November 2011. The severity of psoriasis was calculated using the Psoriasis Area and Severity Index (PASI) [9]. None of the study patients had a PASI score >50. Patients with a PASI score between 0.1 and 10.9 were accepted as mild and those having a score between 11 and 49.9 were considered to be moderate.
Informed consent forms were obtained from every individual included in the study. The study was approved by the local ethics committee.
The exclusion criteria for the study included hypertension, hyperlipidemia, diabetes mellitus, any malignancies, systemic inflammation associated with the disease, previous history of cardiovascular disease, renal and liver insufficiency, severe forms of psoriasis such as erythrodermic psoriasis, systemic immunosuppressive therapy within the last 6 months, smoking, and a Body Mass Index (BMI) >30 kg/m2.
The biochemical parameters were obtained from venous blood samples drawn after an 8-hour fasting period for plasma levels of glucose, high-sensitivity C - reactive protein (hs-CRP), total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, triglycerides, and creatinine. A complete blood count with 6 part differential which included total white blood cells, neutrophils, and lymphocytes was obtained with an automated Sysmex XE 5000 Hematology System (Sysmex America Inc., Mundelein, IL, USA). NLR was calculated as the ratio of the neutrophil and lymphocyte counts [10].
Transthoracic echocardiographic examinations were performed performed with a ViVid 7 Pro (GE Vingmed Ultrasound, Horten Norway). The patients were studied while they were lying in the left lateral position. 3-MHz transducers were used in all echocardiographic studies. LV systolic functions [ejection fraction %, fractional shortening %] and wall motion were assessed using M-mode and 2D. Conventional echocardiography measurements were performed according to the recommendations of the American Society of Echocardiography [11]. We measured Early (E) and Atrial (A) transmitral maximal flow velocities by pulsed-wave Doppler, then, we calculated the ratio E/A and the isovolumic relaxation time was also measured to assess left ventricular diastolic function. Tissue Doppler study was performed utilizing a 3-MHz transducer. Early (E’) and late (A’) diastolic peak annular velocities were measured and the ratio of early mitral flow velocity to the early mitral annular velocity (E/E’) was calculated to assess diastolic function. Systolic mitral annular velocity (Sm) was also measured to assess left ventricular function.
CFR can be measured non-invasively using transthoracic Doppler echocardiography with a high success rate and this technique has been validated against invasive measurements [11,12] with good results. CFR was measured using a high frequency broadband transducer (S8, Philips). All patients were instructed to abstain from caffeine for 12 hours before the examination and oral use of dipyridamole was paused for 72 hours. With the patient in the left supine position the LAD was located as distal as possible using color Doppler either in an apical modified two chamber view or middistal using a modified short axis view. Coronary Flow Velocity (CFV) was measured using pulsed wave Doppler with a sample size of 3–4 mm, at rest and during a 2 minute infusion of adenosine at 0.14 mg kg-1 min-1. The solution was diluted so that the infusion rate was kept at 10 ml min-1. Before and during the adenosine infusion care was taken to maintain the position and angle of the probe, so measurements were done on the same segment of the LAD at the same angle. During the infusion the scale of flow velocity was changed in order to obtain optimal curves for offline measurement. CFR was calculated as the ratio between peaks diastolic CFV during adenosine infusion and during rest using a mean of 3 consecutive cardiac cycles (10 cycles if the patient had atrial fibrillation). Analyses were done offline by an investigator blinded to the other examinations. Blood pressure and ECG were monitored before and during the adenosine infusion. Interobserver variability of CFR was tested on all subjects and the mean difference in CFR was 0.08 with limits of agreement ± 0.22. The Coefficient of Variation (CV), calculated as the within-subject standard deviation divided by the mean of the observations, was 5.5%. Intraobserver variability was tested on 10 randomly selected examinations with a mean difference of 0.04, limits of agreement ± 0.28 and CV 7.5%.
The baseline characteristics of the study population are shown in Table 1. None of the psoriatic patients had severe disease (a PASI score >50). According to basic clinical and demographic characteristics, both groups were similar with regard to age, body mass index, and fasting glucose and cholesterol levels. No significant differences were observed in the systolic or diastolic blood pressures or resting heart rates between the two groups. The mean duration of disease was 10 ± 8 years in the patients with psoriasis. All patients and control-group participants had sinus rhythm and normal 12-lead ECG results [13].
| Psoriasis n = 68 | Control group n = 62 | P-value | |
|---|---|---|---|
| Age (years) | 42.5 ± 12.8 | 43.0 ± 13.2 | >0.05 |
| Sex (male/female) | 46/22 | 45/17 | >0.05 |
| BMI (kg/m2) | 26.9 ± 2.2 | 25.7 ± 2.1 | >0.05 |
| Systolic Bp (mmHg) | 130 ± 10 | 124.6 ± 11 | >0.05 |
| Diastolic Bp (mmHg) | 81 ± 8 | 79 ± 9 | >0.05 |
| Heart rate (beat/min.) | 82 ± 11 | 83 ± 8 | >0.05 |
| Cholesterol (mg/dl) • Total • HDL • LDL |
193 ± 37 45 ± 12 112 ± 35 |
181 ± 32 48 ± 12 105 ± 37 |
> 0.05 |
| Triglycerides (mg/dl) | 149 ± 57 | 143 ± 62 | > 0.05 |
| PASI, mean ± SD | 16.5 ± 15.0 | - | - |
| Duration of psoriasis (years) | 8.3 ± 5.2 | - | - |
Table 1: Demographic characteristics.
Neutrophil-Lymphocyte Ratio (NLR) was significantly higher in patients with psoriasis arthritis than control; subjects (7.86 ± 0.6 vs. 1.39 ± 0.6, P <0 .0001) (Tables 2 and 3). Conventional echocardigraphic assessment showed ejection fraction% and E/A were comparable. On the other hand tissue Doppler study showed significant impaired systolic and diastolic function in patients with psoriatic arthritis compared with control subjects (Sm was 3.9 ± 0.3 vs. 8.9 ± 0.5; P<0.01 and E/E’ was 12.3 + 0.7 vs. 5.3 + 0.8; P<0.01). With respect to CFR analysis, coronary diastolic peak velocities were comparable at rest between patients and control subjects (25.0 ± 6.2 cm/s vs 25.8 ± 5.4, P>0.05), but significantly different after dipyridamole (49.4 ± 10.5/s vs 79.2 ± 13.8 cm/s respectively, p < 0.03). Thus, CFR was (1.9 ± 0.3) in patients with psoriatic arthritis and (3.6 ± 0.2) in control subjects (p<0.002). Of note, analyzing the group with psoriatic arthritis, patients with higher NLR (≥ 3.2) had lower CFR than those with NLR (<3.2) (1.62 ± 0.1 vs. 2.2 ± 0.2; P<0.002). NLR showed high negative correlation with CFR (r=- 0.73, P<0.0001), (Figure 1). It’s glowed a positive correlation with E/E’ (r=0.57; P<0.001), (Figure 2) Negative correlation with Sm (r=-0.43; P<0.03), and positive correlation with hs-CRP (r=-0.49, P<0.03), PASI (r=-0.41; P<0.05), duration of the disease (r=-0.39; P<0.05) (Table 4).
| Psoriasis = 68 | Control group n = 62 | P-value | |
|---|---|---|---|
| Haemoglobin (mmol/l) | 13.45 ± 1.5 | 14.59 ± 1.3 | >0.05 |
| Platelet (mm3) | 233.43 ± 49.00 | 230.45 ± 36.73 | 0.66 |
| White blood cell (103/uL) | 8.50 ± 2.53 | 7.81 ± 1.67 | 0.15 |
| Monocyte (mm3) | 0.54 ± 0.17 | 0.54 ± 0.13 | 0.60 |
| Neutrophil-lymphocyte ratio | 7.86 ± 1.12 | 1.39 ± 0.84 | <0.0001 |
| Glucose (mmol/l) | 5.4 ± 1.2 | 5.1 ± 0.4 | >0.05 |
| Plasma triglycerides | 152 ± 45 | 148 ± 52 | >0.05 |
| Total cholesterol (mmol/l) | 5.56 ± 1.31 | 4.91 ± 1.08 | >0.05 |
| Creatinine (µmol/l) | 74.9 ± 12.1 | 72.9 ± 12.3 | >0.05 |
| hs-CRP (mg/dl) | 3.6 ± 0.2 | 0.8 ± 0.2 | <0.003 |
Table 2: Laboratory investigations.
| Patients N=68 | Control N=62 | P-value | |
|---|---|---|---|
| LVEDd | 46.7 ± 0.84 | 44.1 ± 0.42 | > 0.05 |
| LVESd | 30.2 ± 0.23 | 29.6 ± 0.19 | > 0.05 |
| EF% | 70.6 ± 3.9 | 71.2 ± 3.2 | > 0.05 |
| E/A | 1.1 ± 0.2 | 1.2 ± 0.2 | > 0.05 |
| Sm | 3.9 ± 0.3 | 8.9 ± 0.5 | <0.01 |
| Mean E' cm/s | 6.2 ± 0.6 | 14.5 | <0.02 |
| E/E' | 12.3 ± 0.7 | 5.3 ± 0.8 | <0.01 |
| Baseline DPFV, cm/s | 25.0 ± 6.2 | 25.8 ± 5.4 | > 0.05 |
| Hyperemic DPFV, cm/s | 49.4 ± 10.5 | 79.2 ± 13.8 | < 0.03 |
| CFR | 1.9 ± 0.3 | 3.6 ± 0.2 | < 0.002 |
Table 3: Echocardiograpic data in patients with psoriasis arthritis and control subjects.

Figure 1: Correlation between Neutrophil-Lymhpocyte Ratio (NLR) and Coronary Flow Reserve (CFR) [r= - 0.73; P< 0.0001].
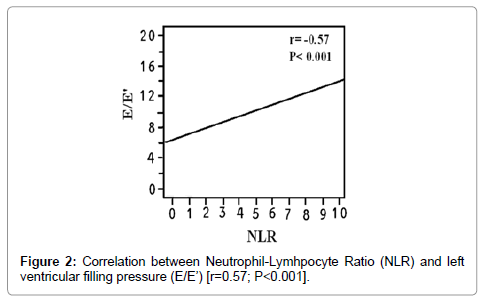
Figure 2: Correlation between Neutrophil-Lymhpocyte Ratio (NLR) and left ventricular filling pressure (E/E’) [r=0.57; P<0.001].
| Variables | r | P value |
|---|---|---|
| Age | 0.19 | >0.05 |
| Body mass index | 0.23 | >0.05 |
| Total cholesterol | 0.27 | >0.05 |
| Triglycerides | 0.24 | >0.05 |
| Duration of the disease | -0.39 | <0.05 |
| PASI | -0.41 | <0.05 |
| Hs-CRP | -0.49 | <0.03 |
| E/E' | 0.57 | <0.001 |
| Sm | -0.43 | <0.03 |
| Neutrophil-Lymphocyte Ratio | -0.73 | < 0.0001 |
Table 4: Pearson Product Moment Correlation between studied variables and coronary flow reserve in psoriatic patients.
Univariate analysis showed that NLR was the most powerful predictor of impaired CFR (P<0.0001) and myocardial dysfunction; (P<0.0001), (Tables 5 and 6). Multivariate regression analysis showed the NLR (P<0.0001) and hs-CRP (P<0.001 and <0.03, respectively) were the two independent predictors of impaired CFR and subclinical LV dysfunction in patients with psoriatic arthritis (Tables 5 and 6).
| Univariate OR (95% CI) | P value | Multivariate OR (95% CI) | P value | |
|---|---|---|---|---|
| Age | 2. 26(0.94-3.95) | >0.05 | 1.92(0.81-3.11) | >0.05 |
| BMI (kg/m2) | 2.35(0.88-4.13) | >0.05 | 2. 15(0.94-3.96) | >0.05 |
| Duration | 4.15(1.22-8.32) | <0.02 | 2. 63(1.015-4.02) | >0.05 |
| PASI | 4.62(1.38-9.51) | <0.02 | 2. 68(1.032-4.21) | >0.05 |
| hs-CRP | 5.15(2.15-9.95) | <0.001 | 3.95(1.45-8.69) | <0.03 |
| NLR | 7.85(3.18-16.33) | <0.0001 | 7.33 (3.65-13.75) | <0.0001 |
Table 5: Independent predictors for impaired coronary flow reserve in multivariate logistic regression analysis.
| Univariate OR (95% CI) | P value | Multivariate OR (95% CI) | P value | |
|---|---|---|---|---|
| Age | 2. 75 (1.05-3.99) | <0.05 | 1.95(0.82-3.25) | >0.05 |
| BMI (kg/m2) | 2.92(1.13-4.42) | <0.05 | 2. 38(0.92-3.76) | >0.05 |
| Duration | 3.86(1.85-8.38) | <0.03 | 2. 45(1.22-3.76) | >0.05 |
| PASI | 4.88(1.48-9.68) | <0.02 | 2. 62 (1.16-4.72) | >0.05 |
| hs-CRP | 5.15(2.15-9.95) | <0.001 | 4.56(1.48-8.99) | <0.02 |
| NLR | 7.42(3.11-17.1) | <0.0001 | 7.35 (3.62-13.82) | <0.0001 |
Table 6: Independent predictors for myocardial dysfunction in multivariate logistic regression analysis.
Receiver operating characteristic curve analysis showed that NLR of ≥ 3.2 was the best cutoff value for the prediction of impaired CFR, with sensitivity and specificity of 96% and 77%, respectively. While NLR of >3.6 was the best cutoff value for the prediction of myocardial dysfunction with sensitivity and specificity of 96% and 77% respectively. The Area Under Curve (AUC) was calculated as 0.912 for CFR (Figure 3) and as 0.825 (Figure 4) for myocardial dysfunction, which indicate good discriminatory powers.

Figure 3: ROC analysis of neutrophil-lymhpocyte ratio (NLR) > 3.2 in prediction of CFR [AUC=0.912; P< 0.001].

Figure 4: ROC analysis of neutrophil-lymhpocyte ratio (NLR) > 3.6 in prediction of E/E’ [AUC=0.825; P<0.001].
The current study demonstrated that coronary flow reserve was significantly impaired in addition to incipient myocardial dysfunction in patients with Psoriatic Arthritis (PsA). The impaired CFR and subclinical myocardial dysfunction were significantly correlated with increased NLR. The interesting finding in the current study is that, NLR was an independent predictor for impaired CFR and incipient myocardial dysfunction in patients with PsA.
Neutrophil-Lymphocyte Ratio (NLR) stands practically for the balance between neutrophil and lymphocyte count in the body, which can also be utilized as an index for systemic inflammatory status Atherosclerosis is a multifocal, smoldering, immune inflammatory disease of medium-sized and large arteries fuelled by lipids. Endothelial cells, leukocytes, and intimal smooth muscle cells are the major players in the development of this disease [14].
The Neutrophil-to-Lymphocyte Ratio (NLR) is an emerging marker for both cardiac and non-cardiac disorders, and recent studies have demonstrated the prognostic value of NLR in stable coronary artery disease [15], acute coronary syndromes [16,17], heart failure [18] as well as patients undergoing Percutaneous Coronary Interventions (PCI) [19].
Increased NLR post-AMI is an independent predictor of major adverse cardiac events in diabetics. Monitoring this easily obtainable new index allows prognostication and risk stratification [20].
Psoriatic Arthritis (PsA) is an immune-mediated inflammatory arthritis associated with psoriasis [21]. Patients with PsA have heterogeneous clinical presentations with diverse articular and dermatological features as well as varied disease course and outcomes. PsA can be a severe form of arthritis with prognosis similar to that of Rheumatoid Arthritis (RA) [22,23]. In addition to skin and musculoskeletal involvement, there is increasing evidence suggesting that patients with PsA also have an increase in risk of cardiovascular disease [24].
Peters et al. [25] demonstrated that the N/L ratios and hs-CRP levels were increasing with increasing in Psoriasis Area and Severity Index score. Furthermore, the N/L ratios and hs-CRP levels of patients were found to be positively correlated and they concluded that the N/L ratio might be a simple, inexpensive and easily assessable marker of systemic inflammation in patients with psoriasis [25].
Systemic inflammation beyond the skin may provide an explanation of the increased cardiovascular risk observed in psoriasis. NLR is potentially an unrecognized predictor of subclinical atherosclerosis in patients with psoriasis [26].
Endothelial dysfunction is considered an early feature in atherogenesis and has been consistently associated with cardiovascular risk [27]. It encompasses an imbalance between vasodilating and vasoconstricting substances, leading to an impaired ability of the artery to dilate in response to physical and chemical stimuli [28]. Postocclusion Flow-Mediated vasodilatation (FMD %) of the brachial artery using ultrasonography is used to noninvasively evaluate endothelial function [29-31]. In the study by Gonzalez-Juanatey et al. [32] in 50 patients with PsA without cardiovascular risk factors or clinically evident CVD, FMD% was found significantly lower in patients with PsA compared with 50 matched healthy controls, indicating endothelial dysfunction in PsA as a potential basis for the association between PsA and atherosclerosis [30,33].
Histologically, psoriasis and atherosclerosis show common features like infiltrating T-cells, monocytes/ macrophages, neutrophils, Dendritic Cells (DCs) and mast cells. The IL-1, IL-6, TNF-α, IFN-γ, CRP and adhesion molecules are synthesized as a result of the inflammatory cascade which is initiated by the introduction of autoantigens to the Th-1 and Th-17 cells. These inflammatory mechanisms seem to be responsible for the formation of the psoriatic plaques and atherosclerosis [31,32].
Utilizing tissue Doppler assessment, we demonstrated that both systolic and diastolic functions were impaired in patients with PsA. Moreover, the myocardial dysfunction was significantly correlated with the NLR.
Results from conventional echocardiography in PsA are controversial. The study by Gonzalez-Juanatey et al. [34] did not find significant subclinical cardiac abnormalities in 50 patients with PsA without clinically evident CVD or atherosclerosis risk factors when compared with 50 matched healthy controls [33]. A recent study by Atzeni et al. [38] reported normal left ventricular wall thickness, size, mass and systolic function using standard 2D echocardiography in 22 patients with PsA when compared with 35 healthy controls [35]. However, the study by Feld et al. [36] found significantly longer PR interval (ms versus ms) on electrocardiogram in 92 patients with PsA compared to 92 matched controls [36]. The abnormal prolongation of the PR interval was asymptomatic, requiring no additional intervention. And there was no statistical difference in the QRS interval or other atrial or ventricular conduction disturbance between patients with PsA and controls [37]. The study by Shang et al., by using both conventional echocardiography and tissue Doppler imaging, found that 65% of 94 PsA patients without established CVD had evidence of subclinical left ventricular dysfunction, significantly higher than that in 63 healthy controls. Diastolic dysfunction appeared (38%) more common than systolic dysfunction (4%) and left ventricular dysfunction was more common in patients with cardiovascular risk factors than in those without [38].
Recently, it was reported that NLR could independently predict CHD mortality in an asymptomatic general population cohort. It reclassifies intermediate risk category of FRS, with significant upward reclassification. NLR should be considered as an inflammatory biomarker of CHD.
Patients with psoriasis arthritis have a significant impaired coronary flow reserve and incipient myocardial dysfunction. Both of which was significantly correlated with Neutrophil-Lymphocyte Ratio (NLR). NLR of >3.2 and >3.6 were the best cut-off values for prediction of impaired CFR and myocardial dysfunction respectively. NLR could be considered a simple non-invasive predictor of future cardiac events in this group of patients.
