Commentary - (2015) Volume 4, Issue 4
Introduction: Systemic Lupus erythematosus (SLE) is characterized by production of antibodies against various cellular antigens derived from nucleus, cytoplasm and cell membrane. Pulmonary manifestations of SLE can include a wide spectrum of diseases such as pleuritis, pneumonia, pulmonary embolism, pneumothorax and pulmonary haemorrhage. Acute lupus pneumonitis may mimic tuberculosis or other acute infectious pneumonia and the incidence varies from 0.9% to 11.7%. We report a case of lupus pneumonitis in a case of SLE mimicking pulmonary tuberculosis.
Case: An 18 year old girl presented with history cough with expectoration with occasional haemoptysis. She also had history of fever, swelling of hands and feet along with hair loss. On examination she was febrile and dyspneic, with moderate to severe anaemia, tachycardia, tachypnoea, and coarse crepitations over the chest. Sputum for acid fast bacilli, bacterial culture and fungal stains were negative. She was initially treated with broad spectrum antibiotics and then empirically with anti-tubercular therapy (ATT). However, as she failed to respond to ATT, further evaluation was done. Anti-nuclear antibodies and ds DNA were strongly positive. Urine analysis showed nephrotic range proteinuria. High resolution computed tomogram of the chest showed bilateral ground glassing suggestive of lupus pneumonitis (LP). A diagnosis of SLE with LP was made and the patient was put on corticosteroids which led to a dramatic response.
Conclusion: SLE has a wide facade of presentations. Keeping this in mind, even in countries where tuberculosis is endemic, the differential diagnosis of SLE and LP should always be considered even where the clinical features and chest X-rays findings are suggestive of pulmonary tuberculosis.
Keywords: Bhattacharya PK, Roy A, Jamil Md, Lyngdoh M, Talukdar KK (2015) Lupus Pneumonitis Masquerading as Pulmonary Tuberculosis – A Case Study. J Arthritis 4:171.
SLE (Systemic lupus erythematosus) is a multisystem autoimmune disorder which has a waxing and waning course. The clinical manifestations of SLE are variable. They include erythematous photosensitive malar rash, oral ulcers, non-erosive polyarthritis or polyarthralgia, polyserositis, immune-mediated cytopenias, renal, neurologic, pulmonary and cardiac abnormalities. Pulmonary manifestations of SLE were first described by Osler in 1904 who described a patient of SLE with persistent lower lobe infiltrates [1]. A wide spectrum of pulmonary presentations has since been described, which include as pleuritis, pneumonia, pulmonary embolism, pneumothorax and pulmonary haemorrhage [2]. Though infections are a frequent cause of pulmonary infiltrates in patients with SLE, in many cases pulmonary infiltrates are not related to infection [1]. Lupus pneumonitis (LP) is an unusual and life threatening complication of SLE usually occurring during SLE flare-ups, but rarely as a presenting feature. Acute LP may mimic tuberculosis or other acute infectious pneumonia and its incidence varies from 0.9% to 11.7% [3]. Hence a high index of clinical suspicion should be kept, when young females present with unexplained pulmonary infiltrates, especially in tuberculosis endemic countries like India where use of empirical antitubercular therapy is high. We hereby report a case of LP as a presenting feature of SLE, thereby mimicking pulmonary tuberculosis.
An 18 years old female was admitted to the hospital with complaints of low grade fever for 2 months, cough with mucoid expectoration for 3 weeks, blood streaked sputum for 1 week and difficulty in breathing for three days prior to admission. She had a history of swelling of hands and feet, off and on, for the past one year although she denied any specific history of joint pain. There was history of irregular menstruation and loss of hair. There was no history of palpitations, breathlessness, weight loss, or exposure to any drugs or toxins. She also gave history of contact with a case of pulmonary tuberculosis in her family. Past medical history was unremarkable and there was no history of travel in the recent past. Her bowel and bladder habits were normal.
On examination she was fully conscious and oriented. Her blood pressure was 100/60 mm of Hg. She had tachycardia (pulse rate 106/ min), tachypnoea (respiratory rate - 26/min) with dyspnoea, as evidenced by the use of accessory muscles of respiration, fever (oral temperature of 1010F). There was presence of pallor and grade-1 diffuse alopecia. On respiratory examination, there were diffuse bilateral coarse crepitations over her chest. Cardiac examination revealed a grade II soft systolic murmur with a prominent pulmonary component of the second heart sound. There were no other positive findings on physical examination.
Chest X-ray showed patchy air space opacification involving bilateral lung fields with right>left, involving all three zones of the lung without any cranio-caudal gradient and cardiomegaly with prominent pulmonary conus (Figure 1). Arterial blood gas analysis showed a pH of 7.3, PCO2 of 48 mmHg, PO2 of 68 mmHg and HCO3- of 28 mmol/L. Her complete blood counts showed a moderate to severe, microcytic hypochromic anemia, leucocytosis with normal differential count and a slightly elevated erythrocyte sedimentation rate (36 mm/hr) (Table 1). Renal functions showed mildly elevated serum urea and creatinine values. Except for a severe hypoalbminemia (1.5 g/dl), her liver functions were within normal range. Serum electrolytes and coagulation profile were within normal range. Urine analysis showed gross proteinuria with occasional pus cells. Sputum for bacteriological culture was sterile, sputum for acid fast bacilli were repeatedly negative. Sputum for fungal stain was also negative. Serological markers for HBV, HCV and HIV were non-reactive. Abdominal ultrasonography revealed mild splenomegaly. Echocardiography showed pulmonary arterial hypertension with a normal left ventricular function. The patient was put on empirical broad spectrum antibiotics (intravenous ceftriaxone 1 g 12 hourly). She was put on high flow oxygen (6 L/min) through face mask and maintained oxygen saturation with high flow of oxygen. However, the patient’s overall clinical condition failed to improve over the next 48 hours. On grounds of prolonged duration of her illness, history of contact with tuberculosis and radiographic findings of multiple pulmonary opacities, the patient was empirically put on anti-tubercular therapy, despite which her clinical condition did not improve over the next two weeks. Further investigations showed positive (4+ speckled) antinuclear antibody (ANA) and anti-ds-DNA (4+) tests, which were diagnostic of SLE. Anti neutrophilic cytoplasmic antibodies (c-ANCA), anti-glomerular basement membrane (anti- GBM) antibodies and rheumatoid factor were negative. Quantitative analysis of urine for protein showed nephrotic range of proteinuria (3.5gm /24 hours). High resolution CT thorax of the patient showed bilateral ground glassing (Right>Left) with relative sparing of the subpleural regions suggestive of LP (Figure 2). Based on these findings and her failure to respond to ATT we made a revised diagnosis of SLE with LP. ATT was stopped and the patient was put on intravenous methyl prednisolone (1,000 mg/day) for three days, followed by oral prednisolone 40 mg/day. There was gradual improvement of the symptoms with disappearance of clinical signs. There was also marked resolution of radiographic findings in the follow up chest X- rays (Figure 3) and improvement of her haematological and biochemical parameters (Table 1). The patient was discharged on steroids on maintenance does and continues to do well in follow up.
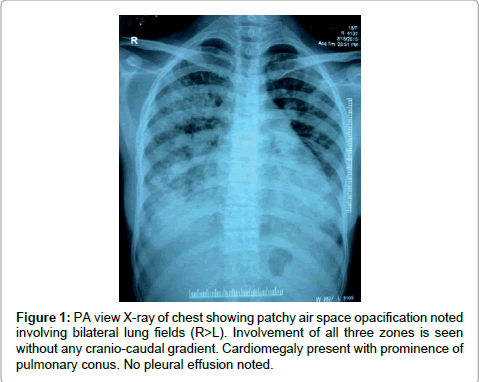
Figure 1: PA view X-ray of chest showing patchy air space opacification noted involving bilateral lung fields (R>L). Involvement of all three zones is seen without any cranio-caudal gradient. Cardiomegaly present with prominence of pulmonary conus. No pleural effusion noted.
| Laboratory parameter (units) | Report | Reference values | |
| On admission | At discharge | ||
| Haemogram | |||
| Haemoglobin (gm/dL) | 6.9 | 8.6 | 12-18 |
| Total Leucocytic count (x103/mm3) | 12.6 | 5 | 4.0 – 11.0 |
| Differential leucocytic count (%) Neutrophil Lymphocyte Monocyte Eosinophil Basophil |
53 37 08 02 00 |
56 40 06 04 00 |
40-75 20-45 2-10 1-6 ≤1 |
| Platelet count (x103/mm3) | 310 | 295 | 150- 400 |
| Erythrocyte Sedimentation rate (mm/h) | 36 | 28 | 0-20 |
| Liver function tests | |||
| Bilirubin (mg/dL) Total Direct Indirect |
0.3 0.1 0.2 |
0.4 0.1 0..3 |
0.3 – 1.3 0.1 - 0.4 0.2 - 0.9 |
| ALT (U/L) | 20 | 22 | 7 - 41 |
| AST (U/L) | 35 | 31 | 12 - 38 |
| Alkaline Phosphatase (IU/L) | 56 | 60 | 30-120 |
| Protein, total (g/dL) | 6.0 | 6.1 | 6.3-8.2 |
| Albumin (g/dL) | 1.5 | 1.8 | 3.5-5.0 |
| Globulin (g/dL) | 4.5 | 4.3 | 1.5-3.0 |
| Coagulation Profile | |||
| Prothrombin Time (s) | 14 | 14.2 | 12.7 – 15.4 |
| INR | 1.22 | 1.24 | 1.34 |
| APTT (s) | 36.2 | 38.2 | 26.3 – 39.4 |
| Renal Profile | |||
| Serum Creatinine (mg/dL) | 1.4 | 0.8 | 0.5 - 0.9 |
| Blood Urea (mg/dL) | 51 | 38 | 10 - 50 |
| Sodium (meq/L) | 136 | 138 | 135-145 |
| Potassium (meq/L) | 3.7 | 3.8 | 3.5-5.5 |
| Calcium (mg/dL) | 9.2 | 9.3 | 8.7 – 10.2 |
| Chloride (meq/L) | 101 | 102 | 90 - 110 |
| Blood glucose, Random (mg/dL) | 103 | 108 | 70 -140 |
| Blood culture | Sterile | Not done | |
| Urine analysis | |||
| RBC (/hpf) | 2-4 | 0-2 | |
| WBC(/hpf) | 1-2 | 1-2 | |
| Protein | 3+ | 2+ | |
| 24 hrs urinary protein excretion (gm) | 3.5 | Not Done | |
| Urine culture | Sterile | Not done | |
| Sputum culture | Sterile | Not done | |
| Sputum for acid fast bacilli | Negative | Not Done | |
| Sputum for fungal stain | Negative | Not Done | |
| Antinuclear antibody (ANA) | Positive (4+) Speckled | Not done | |
| Anti-ds DNA antibody | Positive(4+) | Not Done | |
| Rheumatoid factor | Negative | Not done | |
| c-ANCA | Negative | Negative | |
| p-ANCA | Negative | Negative | |
| Anti-GBM antibody | Negative | Negative | |
| HIV I, II | Non Reactive | Not done | |
| HBsAg | Negative | Not done | |
| Anti HCV | Negative | Not done | |
Table 1: Showing laboratory findings in the patient with lupus pneumonitis.
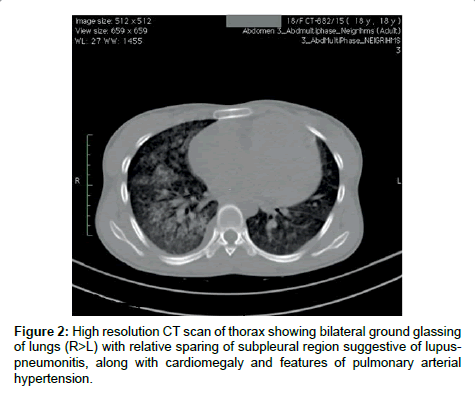
Figure 2: Representative photomicrograph of histopathological features in pulmonary necropsies.
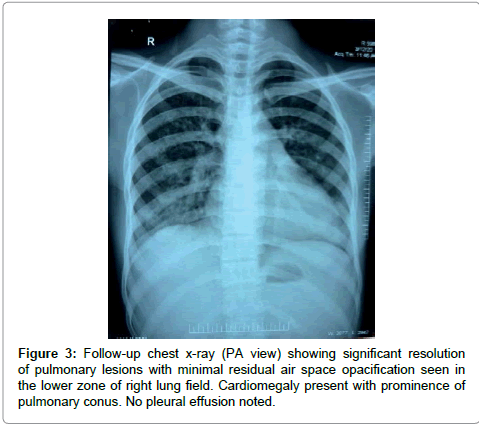
Figure 3: Follow-up chest x-ray (PA view) showing significant resolution of pulmonary lesions with minimal residual air space opacification seen in the lower zone of right lung field. Cardiomegaly present with prominence of pulmonary conus. No pleural effusion noted.
LP is an unusual and life threatening complication of SLE which usually occurs during flare-up but can rarely present as an initial manifestation. LP generally presents with acute onset of fever, cough, tachypnea and hypoxia. The usual radiological features of LP are consolidations in one or more areas usually basal and bilateral and often associated with pleural effusion and pulmonary arterial hypertension [1]. The underlying histology in cases of LP are those of diffuse alveolar damage, bronchiolitis obliterans organizing pneumonia, non-specific interstitial pneumonia, or a combination of these [4]. The mortality of lupus pneumonitis is around 50% with respiratory failure being the primary cause of death [5]. The diagnosis of LP is primarily by exclusion of other causes of lung infiltration such as infective pneumonia (bacterial, mycobacterial, fungal and viral), organizing pneumonia, alveolar hemorrhage, pulmonary embolism, etc. In our case the primary suspicion was indeed of an infective origin, especially tuberculosis, on account of the chronic temporal pattern of the symptoms and signs with a positive history of contact with tuberculosis. However when repeated sputum analysis ruled out a possible infective aetiology the index of suspicion shifted towards other possible causes and finally the diagnosis of LP was established by the clinical manifestations, HRCT findings, anti-nuclear antibody panel and dramatic response to corticosteroids. When connective tissue disorders have a presentation which simulates an infective process the diagnostic challenge to the clinicians becomes manifold. The possibilities of co-existence of a connective tissue disorder with an infection, or an infection which trigger an auto-immune response further complicate the diagnostic process. While on the one hand, patients with SLE can be complicated with superimposed infections, on the other hand, others may present with immune mediated processes which very closely resemble an infectious process, as was found in our case. Pulmonary infections in patients with SLE are also quite common. A previous study reported that pulmonary infections are seen in 20% of cases with SLE [6]. As discussed in our case, it may be difficult to differentiate pulmonary infection from lupus pneumonitis, especially in countries like India which are highly endemic for tuberculosis and there being a resource crunch for carrying out sophisticated immunological tests to diagnose or exclude connective tissue diseases. In such cases, it sometimes becomes imperative to administer broad spectrum antibiotics and also to consider a trial of anti-tubercular therapy prior to establishing a definitive diagnosis. However, other signs of active lupus like rash, arthralgias, oral ulcers, low complement levels, high urinary proteins and casts may help in differentiating lupus pneumonitis from pulmonary infections. The other possibilities that come in the differential diagnosis of lupus pneumonitis are Good Pasteur’s syndrome and Wegner granulomatosis. In our case these entities were excluded on basis on negative c-ANCA and Anti GBM autoantibodies. Because acute LP is a rare entity there is no definite consensus on the modalities of treatment [7]. Patients are generally treated with high dose corticosteroids. In cases which respond poorly to corticosteroids, cyclophophamide has been used to some effect [8].
Connective tissue disorders have a wide facade of presentation. Our case shows a rare presentation of SLE presenting as acute LP which was initially considered as pulmonary tuberculosis. Even in tuberculosis endemic country like India where clinical findings and chest X-rays are taken as sufficient evidence for initiation of anti-tubercular therapy, the differential diagnosis of SLE, especially LP should be borne in mind and appropriate investigations should be carried out so that the possibility of LP is not missed in these patients.
